The respiratory system works with the cardiovascular system to deliver oxygen to the body and remove carbon dioxide. As you know from previous topics, we need to take in oxygen and remove carbon dioxide for aerobic metabolism to work. This produces ATP energy so our muscles and other cells can work.
The process of breathing brings air from the outside into our lungs. In the lungs, oxygen from the air crosses into our bloodstream to be carried throughout the body. When we breathe out, our body releases the carbon dioxide that we have produced. This process requires multiple anatomical structures, which you'll learn about in this topic.
Your body’s cells continually use oxygen for metabolic reactions like nerve transmission, cell-to-cell communication, and muscle contraction. This means that oxygen O2 is always in high demand. Metabolic reactions create a waste product: Carbon dioxide (CO2). CO2 can become toxic to the body's cells when present at high levels. So equally as important as supplying O2, is the respiratory's ability to remove CO2 from the body.
In this topic, you will learn about:
- Respiratory system (an overview)
- Function of the respiratory system
- Respiration at rest and during exercise.
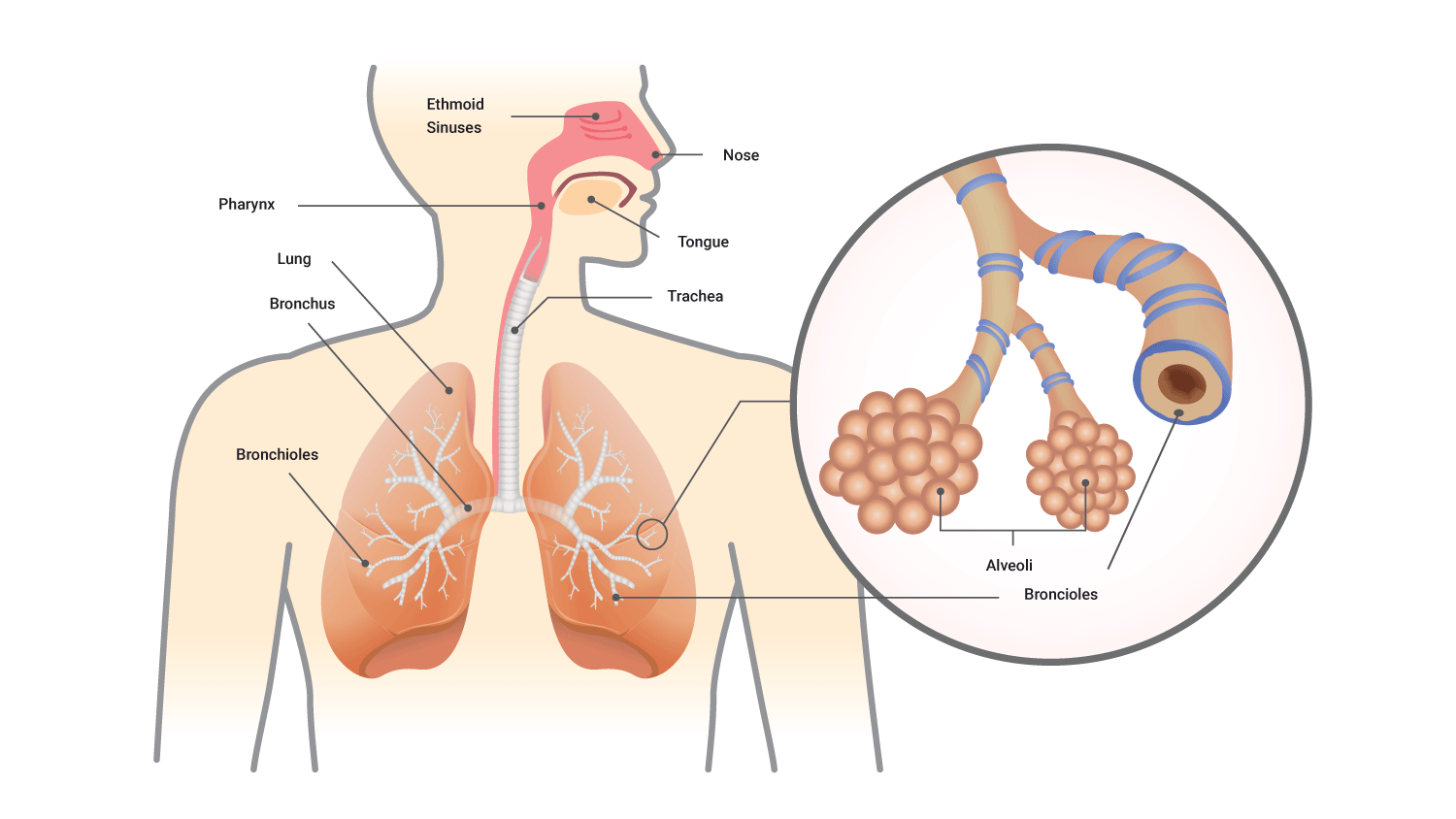
The respiratory system is comprised of the:
- Nose
- Pharynx (throat)
- Larynx (voice box)
- Trachea (windpipe)
- Bronchi (tubular branches which lead to the lungs)
- Lungs

Structural classification
We can arrange the respiratory system structurally based on location.

Functional classification
The respiratory system can also be arranged functionally based on what the parts do.
The conducting zone "conducts" the air in. The structures in this zone provide the passageways for air to travel into and out of the lungs. However, they do a lot more than just conduct. They also moisten, filter, and warm the air we breathe in.

The conducting zone includes:
- Lungs and their network or tubes both inside and outside of the lungs
- Nose
- Basal cavity
- Pharynx and associated structures
- Bronchioles
The function of the conducting zone is to "conduct" the air in. They provide the passageways for air to travel into and out of the lungs. However, they do a lot more than just conduct. They also moisten, filter, and warm the air we breathe in.
The respiratory zone includes structures that are directly involved in gas exchange, i.e., bringing O2 in and CO2 out.

The respiratory zone includes:
- Alveolar ducts
- Alveolar sacs
- Alveoli
Respiratory system structures
Let's look at the main structures in the respiratory system.
Pharynx, larynx, and trachea
The pharynx, larynx, and trachea are part of the conductive zone. They help air travel into and out of the lungs.
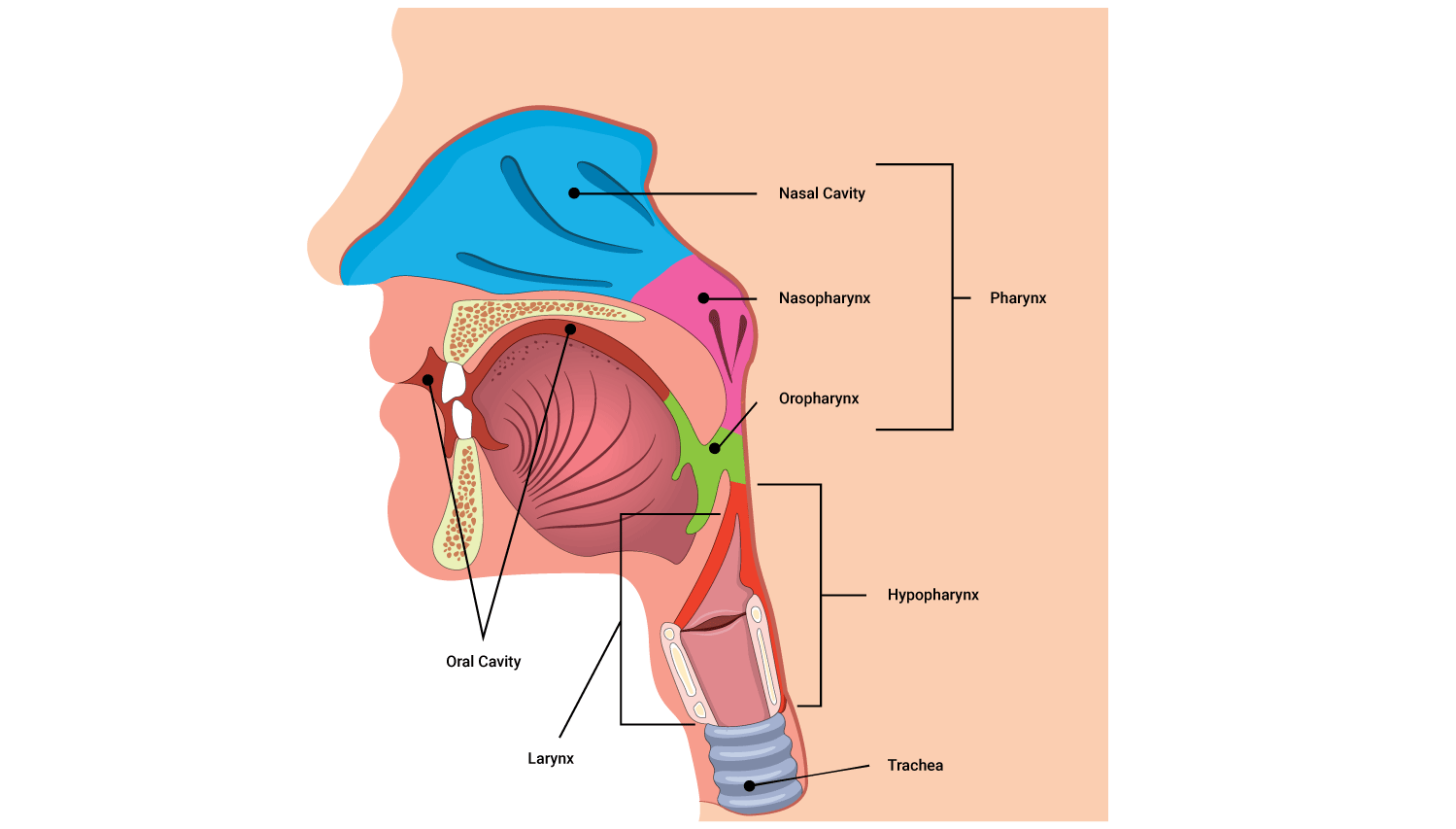
| Pharynx | The pharynx is part of the throat behind the mouth and nasal cavity, and above the oesophagus. It is lined with mucus-producing membranes that help you swallow. |
|---|---|
| Larynx | The larynx is also known as the voice box. It helps produce sound. It also contains the epiglottis, which closes off the windpipe when swallowing. |
| Trachea | The trachea is also known as the windpipe. It allows the passage of air and connects the larynx to the lungs. |
The lungs
The right and left lungs are cone-like structures. They are wider at the bottom where they rest onto the diaphragm, and narrower at the top where they form a point in the collarbone region. The part of each lung that rests on the ribs is referred to as the costal surface of the lungs.
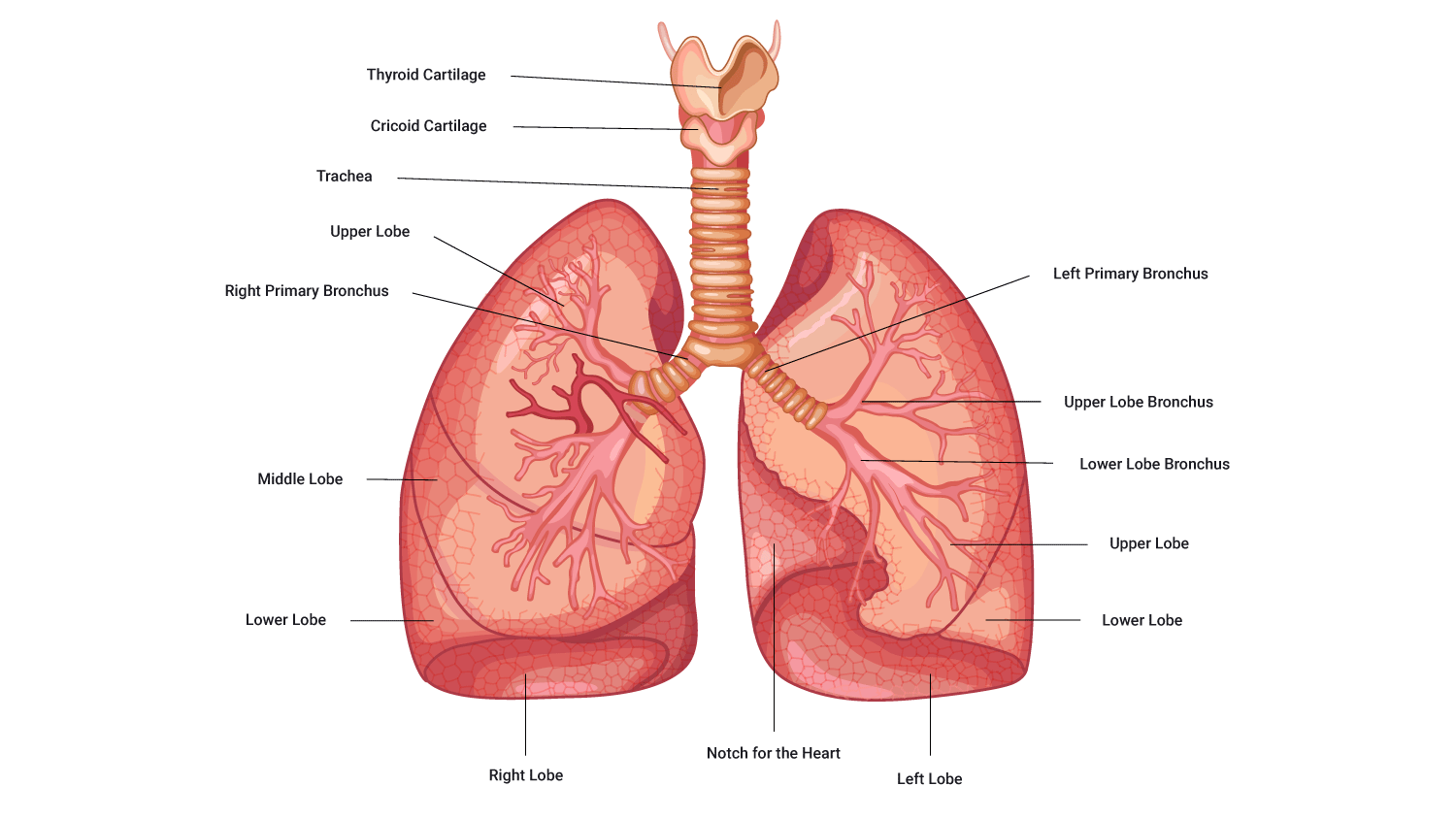
The left and right lungs are structurally different. The left lung is slightly smaller than the right, accommodating the heart in a region called the 'cardiac notch'. The difference in size means the left lung is composed of two lobes (inferior and superior), while the right lung has three lobes (inferior, middle and superior). Remember when we discuss direction in an anatomical context, right and left directions refer to the subject's (client's) right and left.
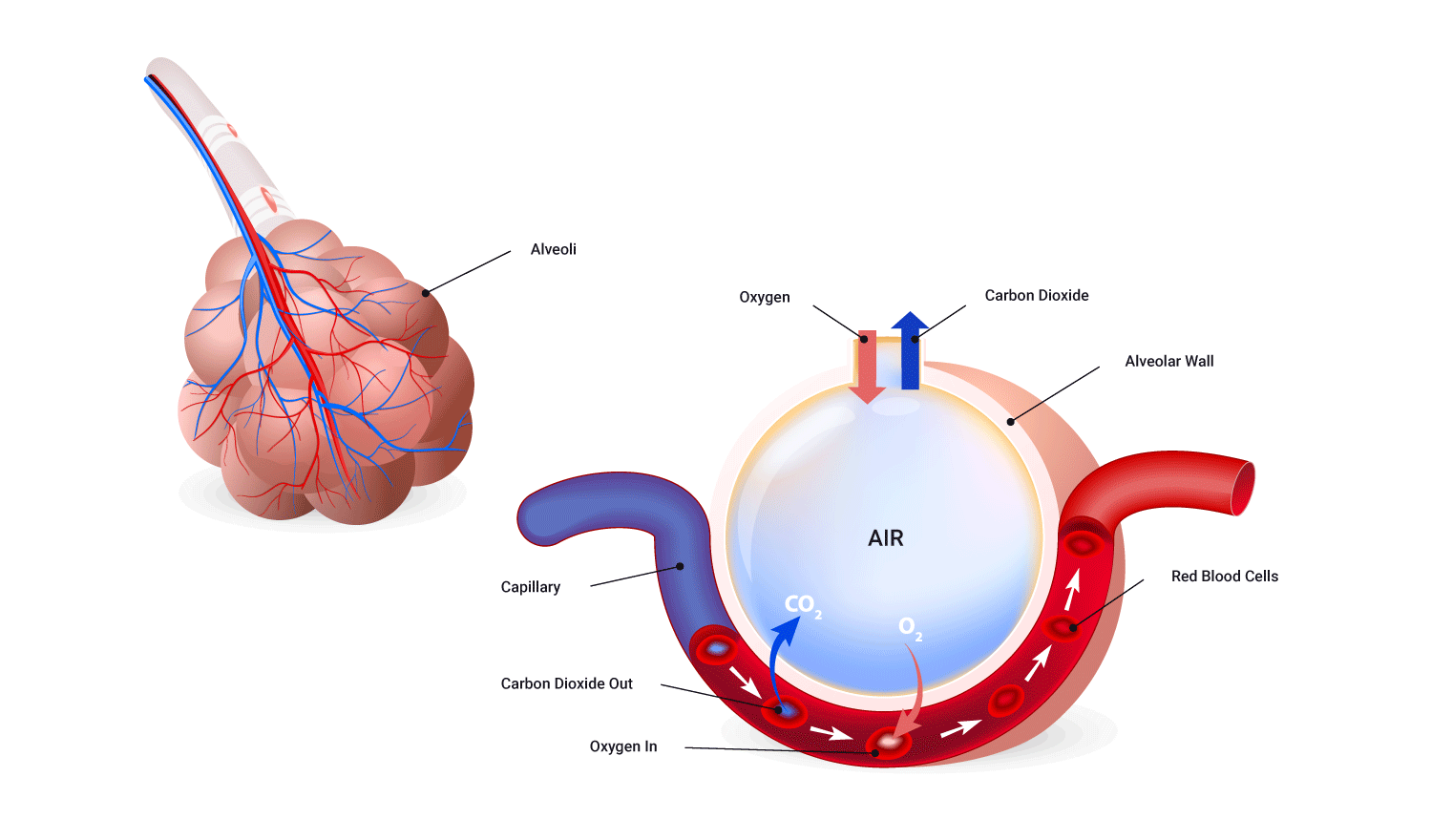
Aveoli
Aveoli are tiny air sacs at the end of the bronchioles. The alveoli are where the lungs and the blood exchange oxygen and carbon dioxide during the process of breathing in and breathing out.
| Alveolar ducts | Each respiratory bronchiole branches off into 2-10 alveolar ducts. |
|---|---|
| Alveolar sacs | The alveolar ducts end with irregularly shaped sacs named alveolar sacs, holding bunches of alveoli in clusters. |
| Alveoli | Individual circular or balloon-like structures are the sites for gas exchange with the blood. |
Watch
The following video shows the relationship and structure of bronchiole, terminal bronchiole, respiratory bronchiole, alveolar duct, alveolar sac, and alveoli.
The lungs are responsible for airflow. But how is airflow established and maintained?
Airflow
There are 2 aspects involved in establishing and maintaining airflow:
- Muscular action
- Pressure differences
The basic rule of airflow is that air will move from an area of high pressure to an area of low pressure. It may help to think of a balloon deflating.
Breathing (also known as ventilation) is the mechanism by which we get air in and out of our lungs. The ability to do this relies on the manipulation of pressure.

Respiratory pressures
In the context of the respiratory system, the pressures that are being referred to are the pressure within the lungs versus the pressure of the external atmosphere (atmospheric pressure). Obviously, we do not have the option to manipulate the atmospheric pressure, but we can manipulate the pressure within our lungs by either increasing or decreasing their size.
- To initiate airflow in (inspiration) it is necessary to lower intra-pulmonary pressure below atmospheric pressure.
- Increasing lung volume (space) reduces intra-pulmonary pressure (pressure in the lungs).
- Decreasing lung volume (space) increases intra-pulmonary pressure.
- To initiate airflow out (expiration) it is necessary to raise intra-pulmonary pressure above atmospheric pressure.
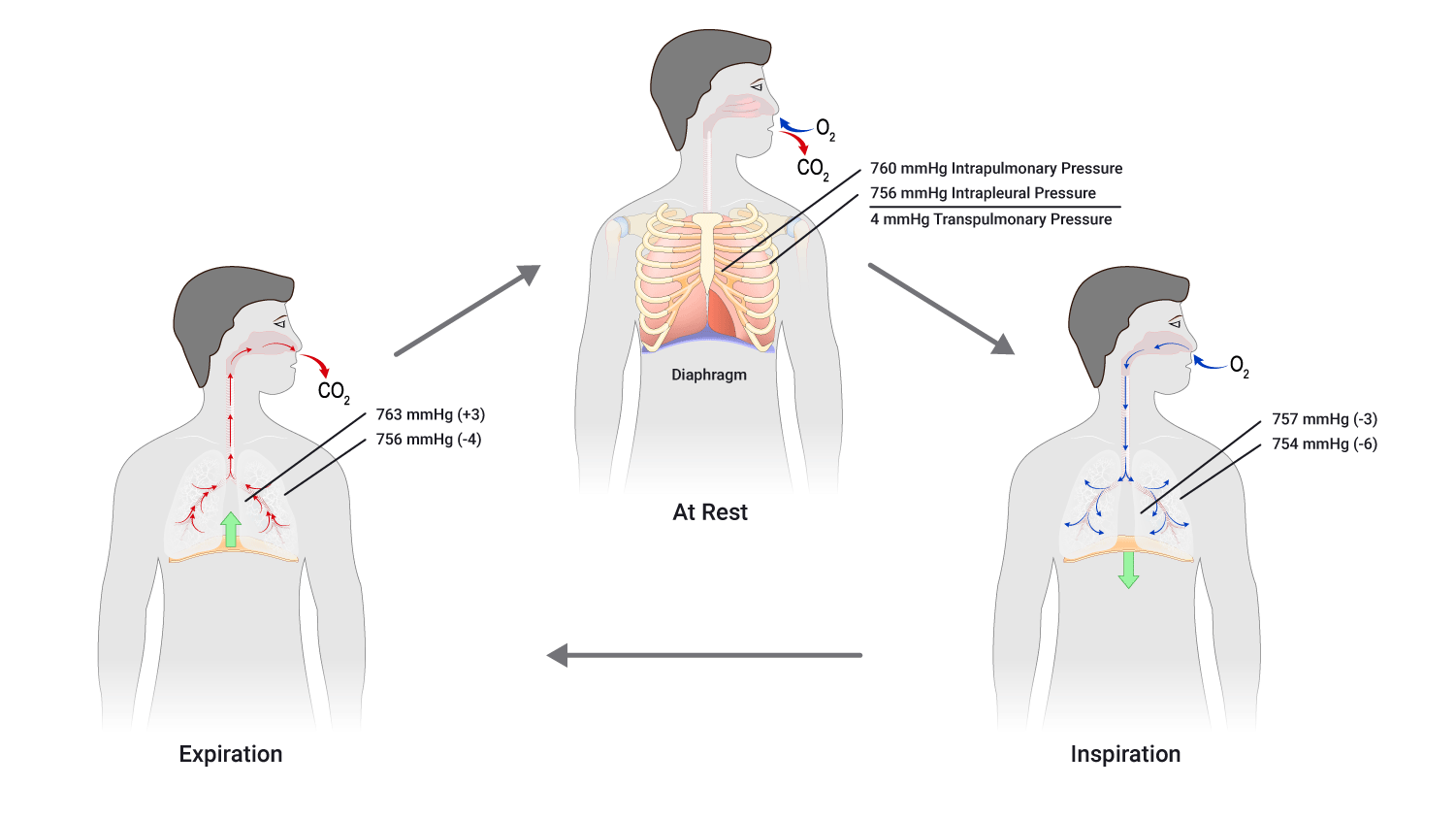
Atmospheric pressure at sea level is around 760 mmHg. To draw air into our lungs, we have to reduce the pressure inside the lungs to below 760 mmHg. To move air out, we need to increase the pressure in the lungs to above 760 mmHg.
The diaphragm
To manipulate lung size and therefore pressure inside the lung cavity, we must recruit muscle to assist. The key muscle involved in breathing is the diaphragm. The diaphragm is a flat, dome-shaped muscle that lies beneath the lungs.

To find your diaphragm, place one hand on your upper belly and give a quick cough. You should feel your diaphragm move.
Expiration and inspiration
Expiration and inspiration are the 2 phases of breathing. Expiration is when gases leave the lungs (expire, exhale) and inspiration is when air flows into the lungs (inspire, inhale). Expiration begins as inspiration ends.
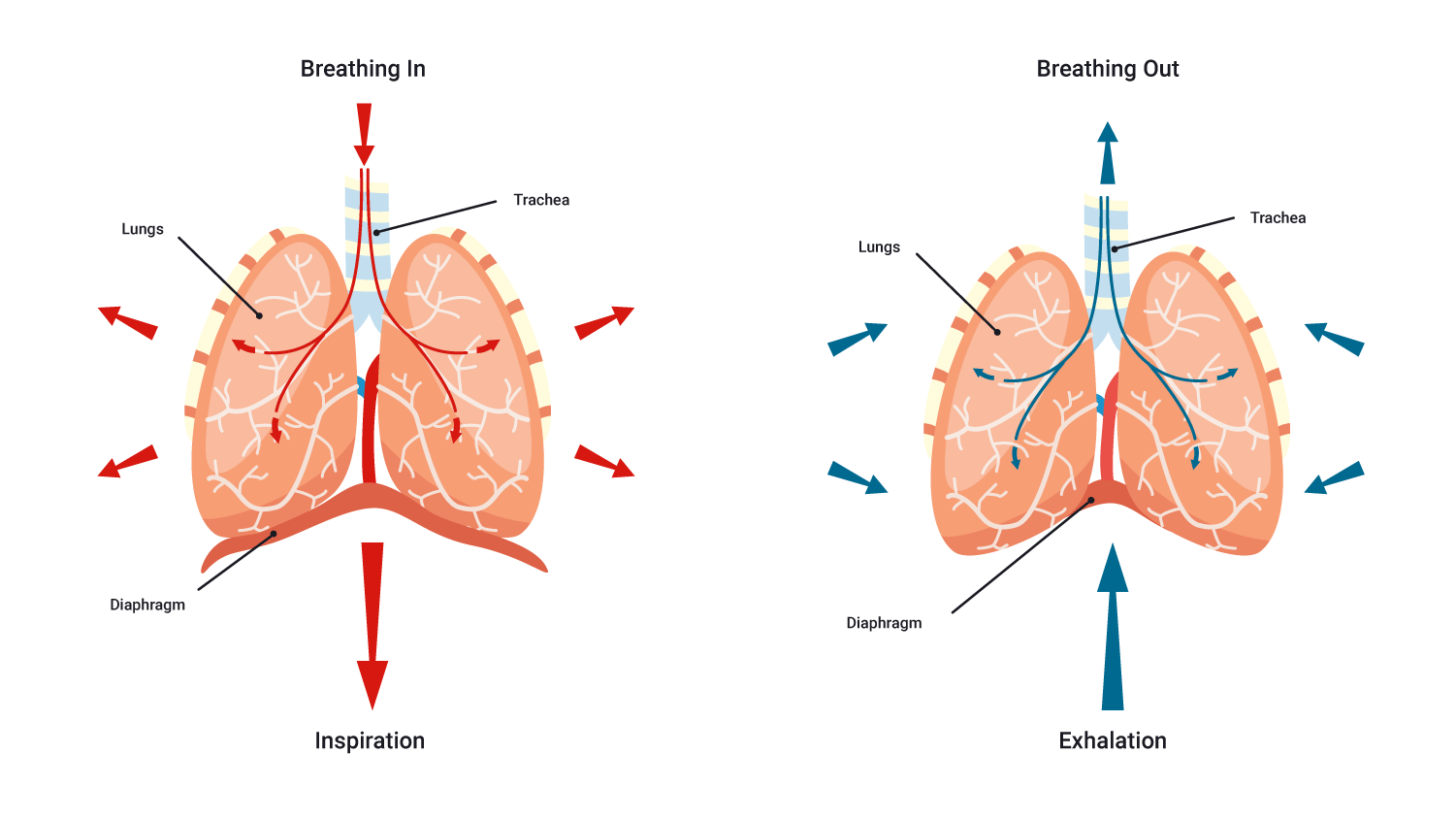
Inspiration, or inhaling, is the first phase of breathing. When the lungs inhale, the diaphragm contracts and pulls downward. At the same time, the muscles between the ribs contract and pull upward. This increases the size of the thoracic cavity and decreases the pressure inside. As a result, air rushes in and fills the lungs.
Expiration also occurs due to a pressure difference/pressure gradient. The pressure in the lungs is greater than the atmospheric pressure so air flows out of the lungs. The diaphragm relaxes, the external intercostals relax, the ribs are depressed. The combination of these results in the volume of the lungs decreasing and the pressure within the lungs decreasing, getting ready for the next inhalation.
An interesting thing to note: In passive/regular expiration, no muscles are used as such. Instead the muscles which were innervated for inspiration to occur simply undergo what is referred to as elastic/muscular recoil and return to their resting position. For this reason, expiration is referred to as a 'passive process' implying no energy is required.
Forced exhalation/expiration
Having said this, expiration can be an active and forced process. This is typically referred to as 'forced expiration'. For example, think about when you have been exercising hard and are breathing very hard, coughing, or playing a wind instrument.
In these situations we see the recruitment of the abdominal and internal intercostal muscles. These muscles contract, increasing the pressure within the abdominal region and thorax, depressing the rib cage and forcing the diaphragm up. This further reduces the volume (and in turn increases the pressure) within the thoracic cavity (in comparison to passive expiration).
Watch
Take a moment to watch the video which provides a brief summary of breathing so far.
Gas Exchange and Transport
Before moving on to gas exchange, let's review what's happening in the conduction zone.
Oxygen is drawn into the lungs because of pressure differences between the atmosphere (outside the body) and the pressure within the lungs, this is known as pressure equilibrium. When the pressure in the lungs is less than the atmospheric pressure it allows for air (including oxygen) to enter the lungs with mechanical assistance from our respiratory muscles.
- O2-rich air is breathed through the mouth or nose. Air is warmed, humidified, and foreign particles are trapped.
- Air travels through the pharynx to the larynx and on through the trachea where more foreign particles are trapped.
- Air enters the primary, secondary, and finally tertiary bronchi and moves through to the bronchioles. Alveoli on the walls of the respiratory bronchioles, alveolar ducts, and alveolar sacs are the site of gas exchange with the blood.

Gas exchange process: Diffusion
When we say gas exchange within the respiratory system, we are referring to the exchange of oxygen O2 and carbon dioxide CO2. The process of gas exchange is known as diffusion.
Diffusion occurs in two phases within the body:
- Between the lungs and blood
- Between the blood and tissues
The rule that governs gas exchange is the same as the one that governs airflow: Gases diffuse from high to low pressure.
Oxygen pressure is represented by the term PO2. It is known as the partial pressure of oxygen. We say 'partial' because oxygen only makes up part of the total air pressure.

Air consists of:
- 78% nitrogen N2
- 21% oxygen O2
- 1% carbon dioxide CO2, argon Ar, and other gases (approximately 0.003% is this is CO2)
At sea level, air has a total pressure of 760 mmHg, so the partial pressure of oxygen (PO2) is:
PO2 = 0.21 x 760 mmHg = 159 mmHg
Phases of diffusion
Now take a closer look at the 2 phases of diffusion.
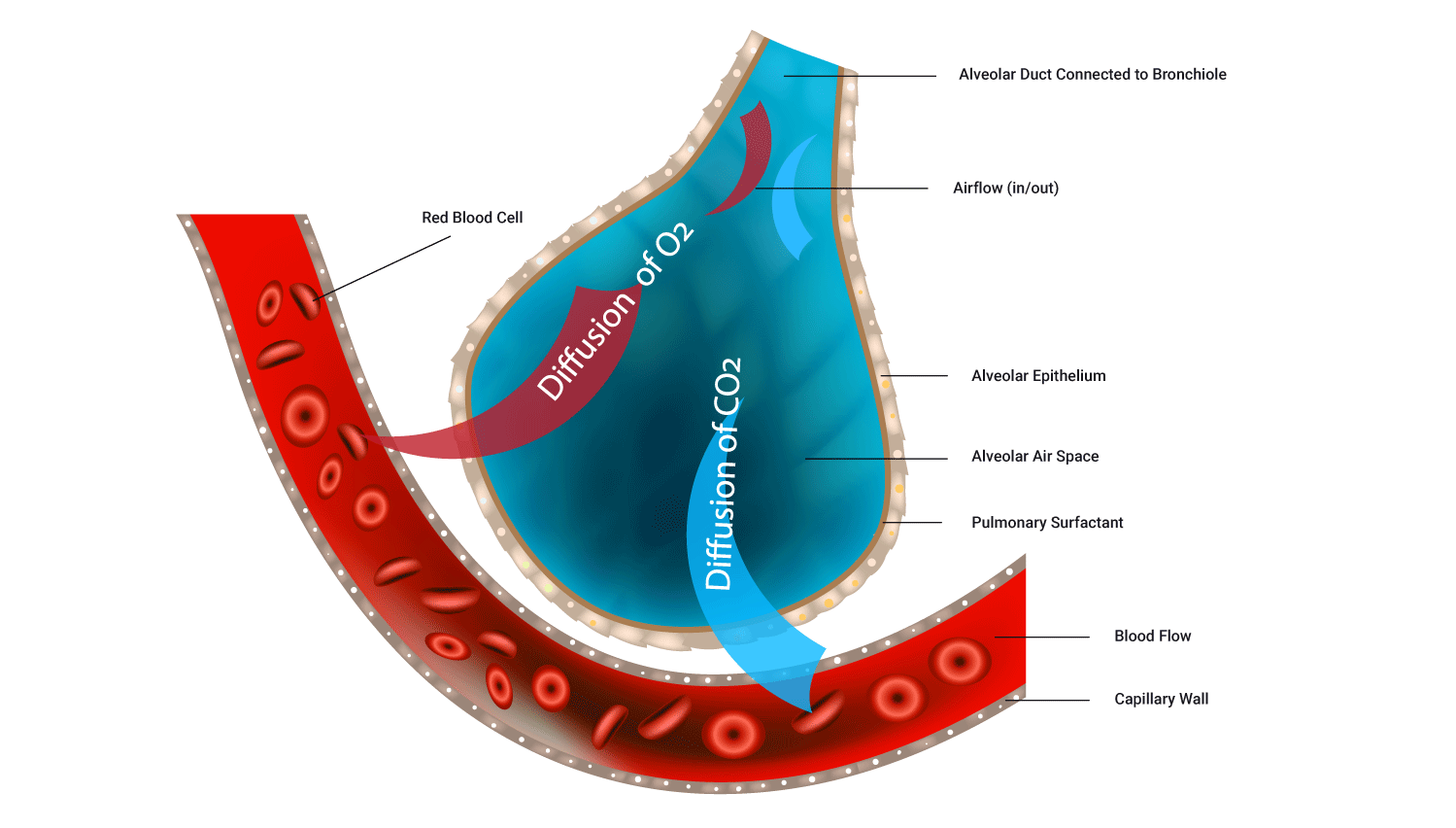
Diffusion of oxygen from lungs (alveoli) to blood (hemoglobin)
For oxygen to move out of the alveoli and into the blood, there needs to be a higher concentration of oxygen in the alveoli than in the blood. Blood returning to the lungs has a lower PO2 as it has delivered some of its oxygen to the body's cells.
PO2 in deoxygenated blood entering the lungs is 40 mmHg (low). PO2 in the lungs, at the alveoli, is 105 mmHg (high), so O2 diffuses out of the lungs into the blood due to the rule of gas flow.
Diffusion of gases between blood and tissues
At tissues (cells), O2 diffuses from the blood to tissues, and CO2 diffuses from tissues to the blood. PO2 in blood reaching the muscles is 100 mmHg (high). PO2 in muscle tissue is 40 mmHg (low).
This means that O2 diffuses from blood to tissues due to the rule of gas flow.
The following image shows the PO2 and PCO2 values at different points along the pathway of blood through the body.

At the body cells, the PO2 has not been stated. It would be 40 mmHg in this instance as gas exchange occurs until gas proportions on both sides are even. As the PO2 in the systemic veins is 40 mmHg, it tells us what the PO2 in the body cells is because O2 would have diffused across the membrane until the concentrations were even in both the blood and cells.
Watch the following video which provides a great overview of gas exchange in the alveoli.
Oxygen transport in blood
Haemoglobin (Hb), present in red blood cells, carries about 98.5% of O2 within the cells of the blood (one haemoglobin molecule can carry four O2). The remaining 1.5% is dissolved in blood plasma.
The O2 carrying capacity of males and females is:
- 201 mL O2/L blood in males
- 174 mL O2/L blood in females
Myoglobin (Mb) is an iron/oxygen-binding protein found in muscle cells that shuttles O2 from the cell membrane to the mitochondria within the muscle cell. Mb has a higher affinity (binding desire, think of stronger magnets) for O2 than haemoglobin, which allows Mb to store a limited amount of O2 'on-site'.
It doesn't take long for haemoglobin to become fully saturated (i.e., carry four O2 per molecule). In times of increased heart rate (e.g., exertion, fright, or illness), red blood cells spend less time at the alveoli, (as little as 0.3 secs), but there is still enough time for haemoglobin to become fully saturated with O2.
Carbon dioxide transportation
As with oxygen, it is only the dissolved carbon dioxide (the smallest percentage of CO2, approximately 7%) that is free for diffusion when it reaches the lungs during expiration.
A greater percentage of carbon dioxide (approximately 70%) is transported in the blood as bicarbonate ions (HCO3-). These ions are broken into three parts when it reaches the alveoli, and once again CO2 is freely available to be exhaled.
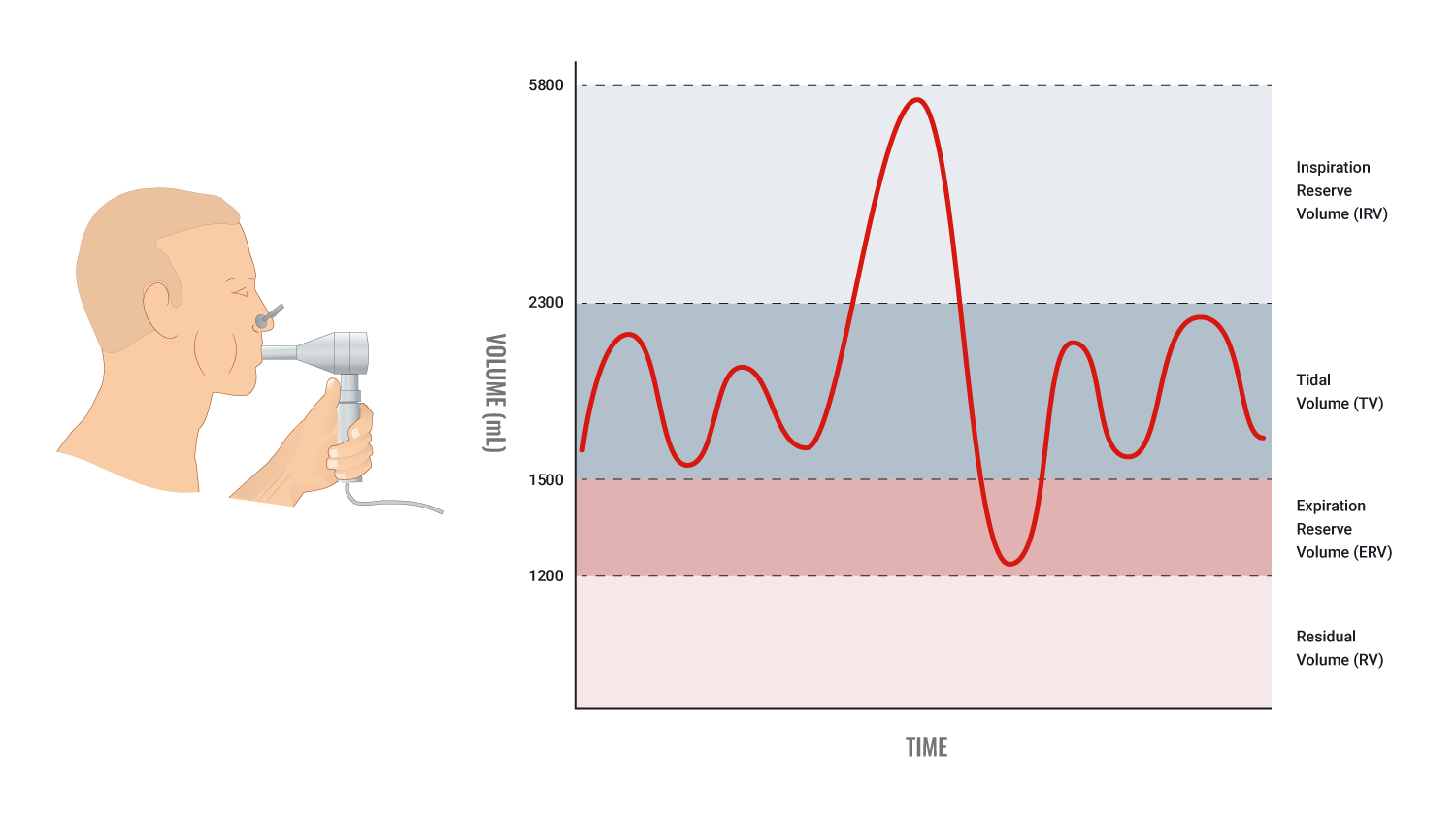
Lung volume is measured by a spirometer and displayed in a graph called a spirogram. The following image shows the typical lung volume of a male (5,800 mL). A female will have a typical lung volume of 4,200 mL.
| Typical lung volumes | Adult male | Adult female | Description |
|---|---|---|---|
| Tidal Volume (TV) | 500mL | 500mL | The volume of air inhaled or exhaled in one breath during quiet, relaxed breathing. |
| Inspiratory Reserve Volume (IRV) | 3,000mL | 1,900mL | The volume of additional inhaled air (when taking a very deep breath). |
| Expiratory Reserve Volume (ERV) | 1,100mL | 700mL | If you inhale normally and then forcibly exhale, the additional air, above the 500mL during quiet, relaxed expiration, is known as expiratory reserve volume. |
| Residual Volume (RV) | 1,200mL | 1,100mL | Even after ERV is exhaled, a large volume of air remains in the lungs. This volume cannot be measured by spirometry. |
| Total Lung Volume (TLV) | 5,800mL | 4,200mL | The total volume of the lungs. |
Lung capacity is determined by combining certain lung volumes. The following table details how to calculate particular lung capacities.
| Lung capacities | Adult male | Adult female | Description |
|---|---|---|---|
| Inspiratory Capacity (IC) | 3,500mL | 2,400mL | IRV+TV |
| Vital Capacity (VC) | 4,600mL | 3,100mL | IRV+TV+ERV Or IC+ERV |
| Functional Residual Capacity (FRC) | 2,300mL | 1,800mL | ERV+RV |
| Total Lung Capacity (TLC) | 5,800mL | 4,200mL | All lung volumes (IRV+TV+ERV+RV) Or IC+FRC |
Exercise and Respiration
Acute effects of exercise on ventilation
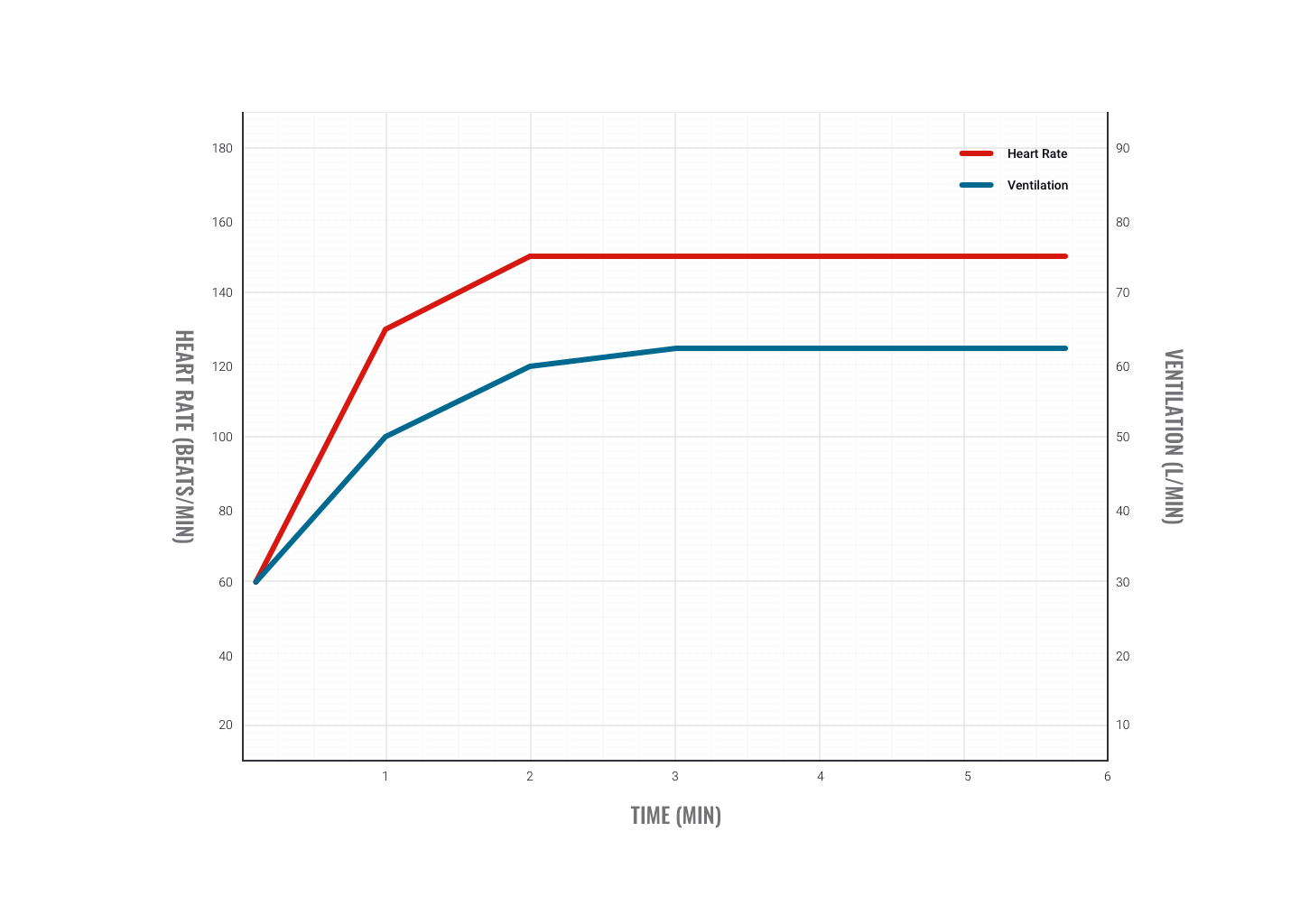
During exercise, ventilation (VE) increases immediately and then levels off at sub-maximal intensities to a steady-state value.
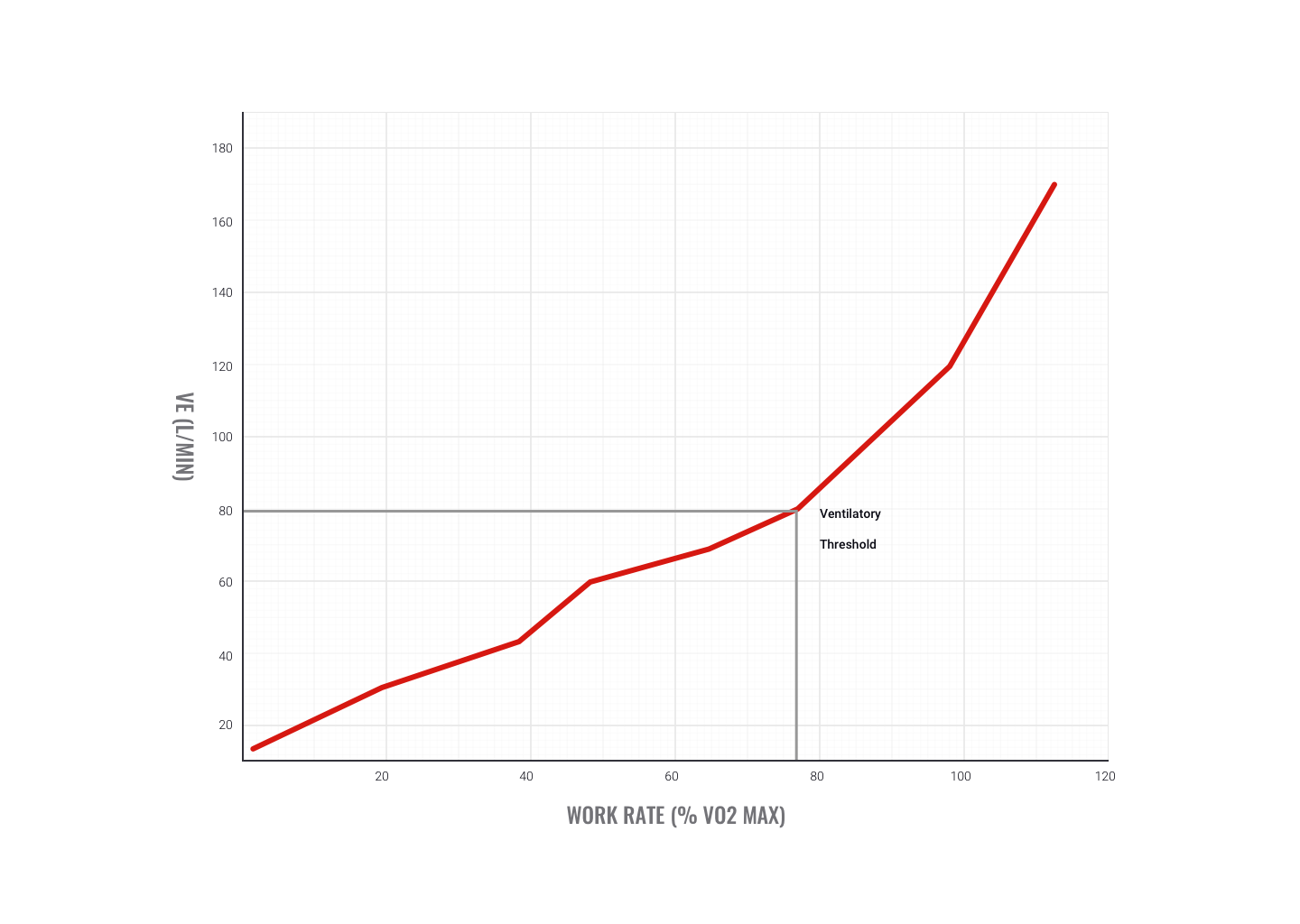
During incremental rises in exercise intensity (for example, raising intensity every minute), ventilation rises linearly in the initial stages. As exercise intensity increases towards maximum, VE increases exponentially. This is called the ventilatory threshold. The fitter you are, the higher the intensity you can work out before reaching this point.
Why does ventilation increase during exercise?
Muscle metabolism increases due to an increased demand for work. Metabolism requires O2, so greater amounts are required. CO2 is a by-product of aerobic exercise, therefore the demand for CO2 removal is also increased.
Heart rate (HR) increases to match the gas and nutrient delivery needs of working muscles and to transport waste away from muscles. This triggers an increase in breathing reserve (VE) to provide the increased requirement of O2 and eliminate the increased amounts of CO2 produced.
The ventilatory threshold indicates the needs of muscle are no longer being met and the ventilation rate increases sharply in an attempt to off-load greater amounts of CO2 production. This strongly indicates that a switch from aerobic to anaerobic energy system use has occurred.

How does the brain know to increase breathing during exercise?
The respiratory system relies on the central and peripheral chemoreceptors (chemical messengers), which give input to the respiratory control centre in the brain (hypothalamus).
- At rest, 'neural' input is sent to the control centre to stimulate the desire to breathe.
- During exercise, the information from 'humoral' chemoreceptors (gathering information from blood) is of greater importance.
Increases in breathing depth are usually in response to increased O2 demand in the body. Increased breathing rate is more likely to be in response to increasing CO2 levels within the blood.
Receptors involved in ventilation
Central and peripheral chemoreceptors are involved in the respiratory system,
- Central: These are located in the medulla (brain stem) and stimulated by changes to PCO2 in spinal fluid. They send messages to the respiratory control centre to increase the ventilation rate.
- Peripheral: These are found in the aorta and carotid artery and respond to increases in H+ and PCO2 in arteries. They send a message to the respiratory control centre to increase the ventilation rate.
Hyperventilation
Hyperventilation refers to an increased rate of ventilation in excess of what is required by the body. This results in CO2 being expelled/removed at a rate faster than the body is producing it. This lowers CO2 levels in the blood and lowers pH.
Changes to blood pH can have serious effects and will have a negative effect on gas exchange. This is why it is important to try and regulate your breathing during exercise.
The method of breathing into a bag is thought to be effective as it recirculates CO2 back into the body.

Chronic effect of aerobic training on ventilation
Improvements in ventilation efficiency are mainly due to improved strength of breathing muscles, enhanced elasticity of the lungs, and higher red blood cell counts. This leads to the following improvements:
- Increase in maximum pulmonary ventilation, i.e., an increased amount of air in and out of the lungs.
- Increase in maximum pulmonary diffusion, i.e., a more complete exchange of gas from alveoli to blood and from blood to tissues.
- Increase in a-VO2 diffusion, i.e., more O2 carried per litre of blood. Therefore at sub-maximal exercise rates, the heart doesn’t have to work as hard to deliver the same amount of O2.
Increased aerobic fitness leads to a lower breathing rate at any intensity following training. This may also be due to lower blood lactic acid levels (enhanced waste removal due to cardiovascular improvements). This results in less feedback to stimulate breathing (that is, to remove waste).
Check that you have a good grasp of the respiratory system before attempting your assessment and moving to the next topic.
Watch
This slightly longer video provides a fun and informative overview of respiration and gas exchange. Not all of the information is required at this stage however, understanding the process behind gas exchange and the effects of hyperventilation will provide dividends to your programme design and client care. There is also a 'Part 1' which you may wish to view in your own time.
