
As a Personal Trainer, you will have different objectives for your clients. Objectives are designed to achieve agreed-upon fitness outcomes consistent with exercise technique standards. These fitness plans for clients may include increasing endurance, muscle building, pain reduction and weight loss.
Prior to achieving any of the client's fitness goals/objectives they must first be able to complete basic functional movements, undertake a variety of assessment and monitoring activities, and have any associated risks and adaptations explained to them.
There will be different physiological adaptations based on short-term and long-term exercise programs as well as a result of different environmental conditions. It is important that you are familiar with these adaptations so you can plan a more productive exercise program and also explain the changes to the client.
Movement is affected by various types of forces which impact and guide direction. This reaction is usually in the form of a push or pull movement as a result of an interaction between two objects.
In regards to human body functional movement is exerted by either internal or external forces:
-
Internal - Muscles pulling (flexing) or pushing (extending) joints.
-
External - Gravity pulling us towards the ground and occasionally other forces which have a push effect such as the wind.
The push and pull motion can be broken down into five specific movements:
-
Compression - Occurs when a force pushes on an object. For example, bodyweight being pulled by gravity results in certain bones being pushed closer together (particularly the vertebrae in the spine) and thus we are taller at the beginning of the day and slightly shorter at the end of the day, before the compression is eased by laying down in bed.
-
Tension - Occurs when a force pulls on an object. Imagine fencing wire being pulled very tightly between the posts.
-
Bending - Simultaneous pulling (tension) and pushing (compression).
-
Torsion - Occurs when one end of an object is fixed and the other end twists around an axis. For example, twisting an ankle.
-
Shear loads - Extreme version of bending and can also be caused by impact with another object. If a shear load is applied to a human body it often causes a fracture to occur.
There are seven basic movements that the human body can perform, these actions underpin all other exercises.
Moving a weight away from your body or moving your body away from a fixed surface, for example, the floor when doing a push-up.
Example of push exercises include:
-
Chest press.
-
Incline press.
-
Shoulder press (overhead press).
-
Push-up.
-
Floor press.
-
Tricep dips.
-
Handstand press-ups.
Muscles that are utilised when undertaking push exercises include the pectorals, triceps, fronts of shoulders, and quadriceps. Progression is usually achieved by increasing the amount of resistance (weight).
One of the most common push exercises is the push-up. To determine functional movement capability in a client whilst they are undertaking a push-up follow these steps:
-
Hands should be wider than shoulder-width apart.
-
The client should lower 90 degrees at the elbow and press back up to starting position, repeating at least five to 10 times.
Look for back swaying, scapular stability or scapular winging and symmetry during both the eccentric (muscle lengthening in response to force) and concentric (muscle shortens) phase.

Another common push exercise is the overhead press (or shoulder press) where a weight is pressed straight upwards from racking position until the arms are locked out overhead.
Muscles that are utilised when undertaking push exercises (in particular overhead press) include the pectorals, triceps, deltoids, and trapezius muscle. Progression is usually achieved by increasing the amount of resistance (weight).
To determine functional movement capability in a client whilst they are undertaking an overhead press follow these steps:
-
Client's feet and hands (gripping the bar) should be shoulder-width apart.
-
Start with the bar high against the chest.
-
Back should be straight, knees and hips locked. Gluteal muscles can be squeezed.
-
Head is tilted back slightly to allow the bar to pass overhead.
-
Bar is raised until the elbows lock.
-
Lower the bar and then repeat.
Focus on the coordination of movements particularly variances of shoulder joints, which are susceptible to injury and imbalances. Lifters often develop imbalances that make one side of a joint stronger and tighter than the other, resulting in chronic pain.

Bringing a weight towards your body or pulling your body towards a fixed surface, for example a bar when undertaking a pull-up.
Examples of pull exercises include:
-
Pull-up.
-
Bent over row.
-
Upright row.
-
Seated cable rows.
-
Lat pull down.
-
Inverted rows.
-
Rear shoulder flys,
-
Bicep curls.
Muscles that are utilised when undertaking pull exercises include the back muscles, biceps, hamstrings, obliques and trapezius.
A specific example of a pull exercise is the seated cable row. To determine functional movement capability in a client whilst they are undertaking a seated cable row follow these steps:
-
The client should sit upright at the machine with feet either on the floor or on the foot pads, knees bent.
-
Pull elbow towards the torso until handles reach the abdominals.
-
Hold for one second.
-
Return to starting position.
Observe whether shoulders are down and the client’s ability to retract shoulder blades. Watch for activation of muscles, such as lats (latissimus dorsi), rhomboids, mid traps (trapezius), control through concentric and eccentric phases of contraction, and symmetry on both sides of the body.
Another common pull exercise is the overhead pull whereby a dumbbell is pulled up from behind the head and held in an overhead position whilst laying on the ground or on a bench.
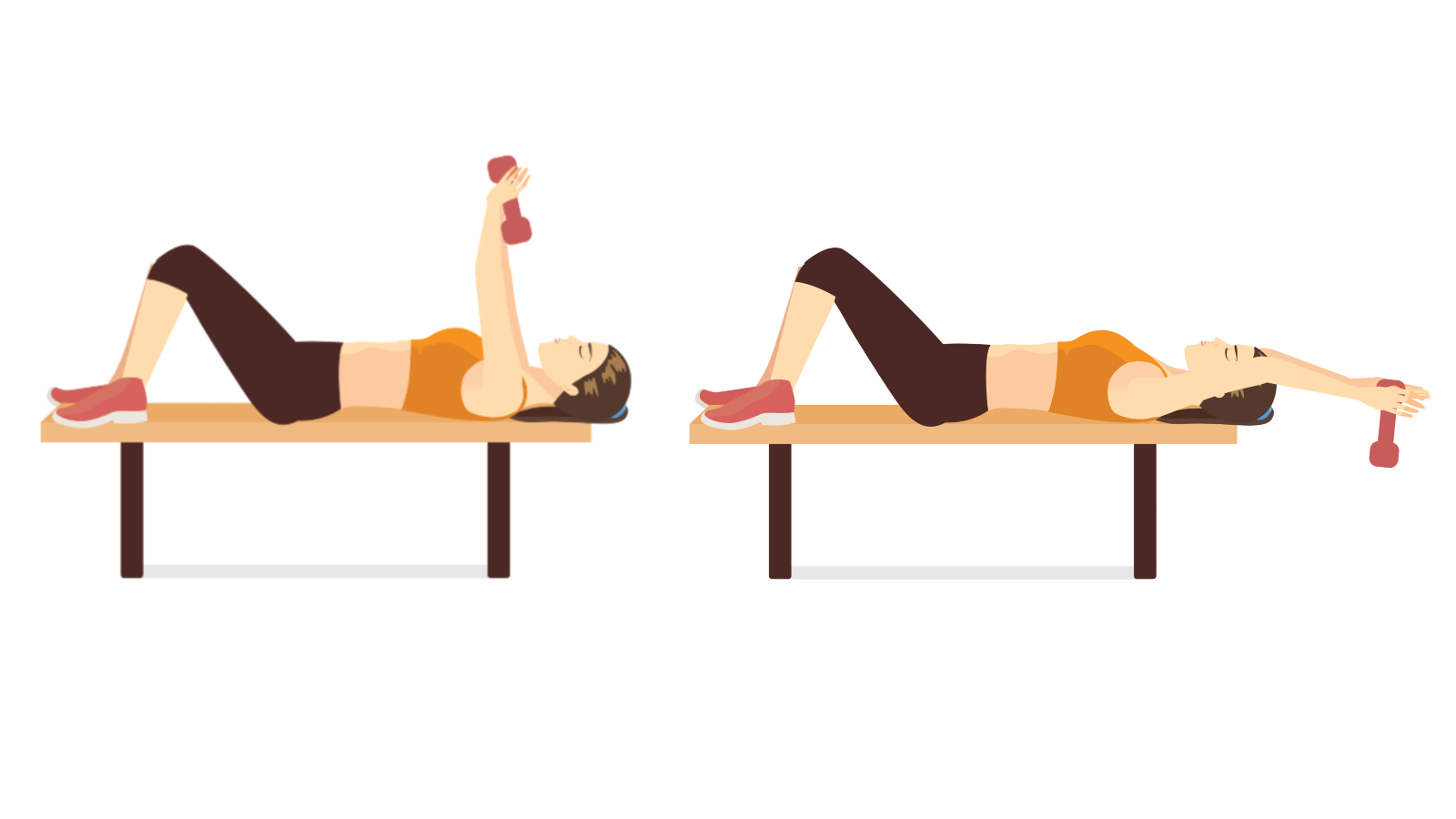
Muscles that are utilised when undertaking overhead pull exercises include the triceps and shoulder muscles. Progression is usually achieved by increasing the amount of resistance (weight).
To determine functional movement capability in a client whilst they are undertaking an overhead pull using dumbbells follow these steps:
-
The client should lie on their back with knees bent and feet on the floor.
-
Arms should be extended above the chest.
-
Engaging the abdominals, the dumbbells should be lowered past the head keeping the arms mostly straight with elbows slightly flexed. Dumbbells should not touch the floor.
-
Raise the dumbbells back to the starting position.
Note the client's lower lumbar region. The lower back should stay firm against the floor throughout the movement. Observe for symmetry and engagement of triceps muscles and shoulder joints.
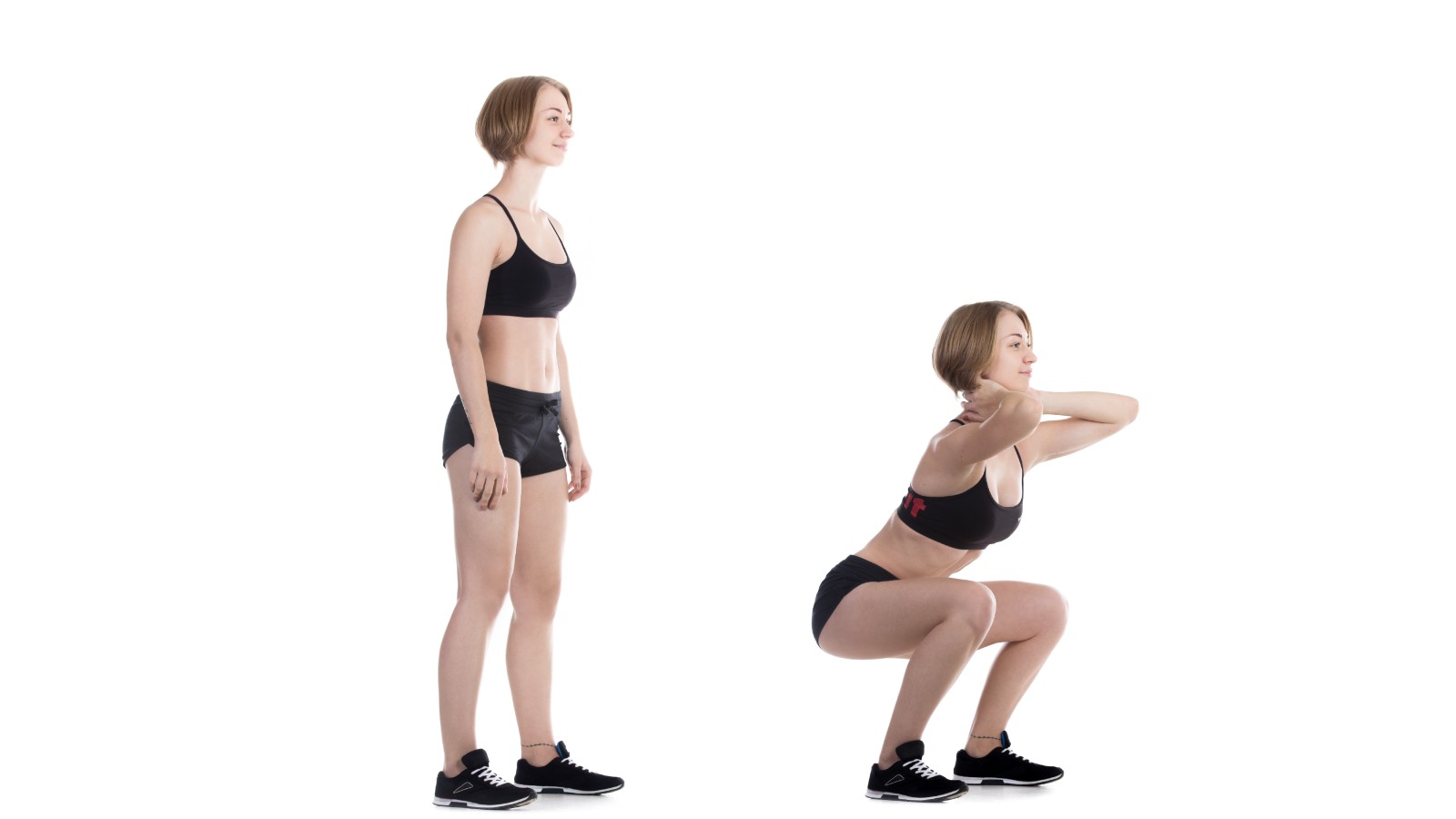
Bending at the knees to lower the body down towards the floor, a similar motion that one undertakes when sitting down on a chair and standing back up again, however, without the chair. The squat involves the hip and knee joints.
Examples of squat exercises include:
-
Standard squat without added weight (utilising body weight only).
-
Jump squat.
-
Barbell squat.
Muscles that are utilised when undertaking squat exercises include the quadriceps, hamstrings, gluteal muscles, abdominals, calves, and back muscles (especially when undertaking barbell squats).
To determine functional movement capability in a client whilst they are undertaking a standard squat exercise follow these steps:
-
Feet should be slightly more than shoulder width apart and toes pointed slightly outward.
-
Client's head, neck, and back should be straight, and pelvis back.
-
Lower into squat position until thighs are parallel with the floor.
-
Return to starting position.
Take note of any asymmetries, compensation, and weaknesses in quadriceps, hamstrings, and lower lumbar region.
Positioning one leg forward with the knee bent and the other leg positioned behind in an exaggerated stepping motion. Body weight is then lowered until the forward leg is parallel to the floor and the shin is vertical.
Examples of lunge exercises include:
-
Stationary lunge.
-
Side or lateral lunge.
-
Walking lunge.
-
Reverse lunge.
-
Twist lunge.
-
Curtsy lunge.
Muscles that are utilised when undertaking lunge exercises include the abdominals, back muscles, gluteal muscles, quadriceps, hamstrings, and calves.
To determine functional movement capability in a client whilst they are undertaking a stationary lunge exercise follow these steps:
-
Client's feet should be hip width apart, then they take a large step forwards with one foot into the starting position. The front knee should line up with the ankle.
-
Weight should be in the heel of the front foot and on the ball of the back foot.
-
The client should slowly lower the back knee toward the floor (approximately 90° angle), then return to a starting position, before repeating.
-
Complete lunge exercises for each leg.
Focus on hip, knee and ankle alignment, internal and external rotation of the hip. Strength limitations and imbalance may include: the front knee sliding forward beyond the toes, the front heel lifting up, and stabilising issues. Compare, if there is a difference on each side.

Bending at the hips (moving in and out of flexion), whilst keeping a straight spine. For example, when picking something up from the floor.
Examples of hinge exercises include:
-
Standard hip hinge (with or without dowel).
-
Barbell deadlift.
-
Kettlebell swings.
Muscles that are utilised when undertaking hinge exercises include the gluteal muscles, hamstrings, quadriceps, lower back, and core muscles.
To determine functional movement capability in a client whilst they are undertaking a dowel hip hinge exercise follow these steps:
-
The client should be standing with feet slightly wider than shoulder distance apart. Toes pointed slightly outward.
-
Have them hold a piece of dowel or broom handle against their back, grasping one end with the right hand, in the natural curve of the neck, and the other end with the left, in the small of the back.
-
Weight should be shifted to the heels and hips pushed backwards.
-
The torso is lowered until its midway between vertical and parallel to the floor. Knees should have a slight bend during this process. The dowel or stick is held against the back during this process.
-
Reverse the movement.
The dowel or stick should be touching the back of the head, the upper back, and the sacrum (where the lower back meets the buttocks) throughout the hinge movement, if the dowel or stick looses contact with these points then the move is being done incorrectly.
Twisting the torso from side to side at the core. Often performed using cables or resistance bands.
Examples of rotation exercises include:
-
Sledgehammer swings.
-
Cable woodchoppers.
-
Medicine ball rotational throws.
Muscles that are utilised when undertaking rotation exercises (in particular cable woodchoppers) include the obliques and the transverse abdominis muscle.
To determine functional movement capability in a client whilst they are undertaking a cable woodchop exercise follow these steps:
-
Client should grasp a D-shaped handle affixed to a cable pulley at hip height.
-
Hands should be interlocked.
-
They should be standing sideways to the machine with feet shoulder width apart, toes facing away from the cable machine, and knees slightly bent.
-
Client should be looking away from the machine (in the same direction the toes are pointing).
-
Client then pulls their arms across the torso in a straight line, until the hand closest to the machine is past the shoulders.
-
Reverse the sequence and repeat.
-
Switch sides and undertake rotation.
Common mistakes include arching the lower back and twisting the body out of alignment. Movement should NOT be initiated through the hip.
Locomotion of the body from one point to another. This is probably the most well known and commonly used functional movement, it includes:
-
Walking.
-
Running.
-
Jogging.
-
Hurdle step.
Progression can be achieved by adding weight (load) during the gait or increasing the distanced walked / run.
Muscles that are utilised when undertaking gait exercises include the hip extensors, hamstrings, quadriceps, calves, and gluteal muscles.
To determine functional movement capability in a client whilst they are undertaking a gait (walking) movement ensure the following:
-
Client should be pushing forward from the hips to initiate the first step.
-
They should be maintaining free hand / arm swing, with slight hip rotation, in coordination with leg movements.
-
They should maintain good posture and NOT be leaning forward.
-
Feet should roll through the stepping motion, from heel to toe, and NOT slap down flat.
Clients will utilise these functional movements in different quantities depending on their chosen exercise regime / sport. For example, runners will predominately use the gait and the lunge movements whereas a weight lifter will use the squat, pull, and push movements.
However, clients should be able to perform all seven of the functional movements to some degree without pain or discomfort. If pain is felt or if the client is unable to complete any of the movements then the term 'dysfunctional movement' is used.
The inability to undertake some or all of these functional movements can be caused by a variety of conditions, some of which are chronic diseases/syndromes. It may not be possible to correct these dysfunctions through physical exercise (although improvements or reduction in pain may be possible with certain exercises), and a referral to a medical or allied health professional may be required.
Poor posture can also negatively influence some or all of these functional movements and this is an area where certain exercises can help.
Key terms for balancing exercises are used to describe variation of stance:
-
Bilateral – Two legs planted (includes narrow, wide, lunge, tandem).
-
Tandem – Specifically one foot planted directly in front of the other foot, heel near or against toe.
-
Single Limb – One leg planted on surface only.
Below are some examples of balance assessment activities that can be undertaken with clients. Not all of the activities are required for every client, professional judgement is required to summarily assess the client's basic ability and choose appropriate activities. The exercises should start out easy and become progressively challenging over the course of the regimen.
-
Gradually remove upper extremity support.
-
Make the seating surface less stable – ie. therapy ball.
-
Modify lower extremity support – ie. sitting cross-legged, one leg up.
-
Modify trunk support – ie. not using chair backrest to lean on.
-
Add upper extremity activities – ie. reaching, throwing.
-
Add manual resistance.
-
Add visual challenges and head movements.

-
Decrease the level of assistive device used: parallel bars, walker, cane, and no device.
-
Move from bilateral stance to single limb stance.
-
Add upper extremity or functional activities.
-
Make the standing surface less stable.
-
Add vertical changes to the standing surface – ie. steps.
-
Increase the distance moved away from midline.
-
Change the speed of movement.
-
Add manual resistance.
-
Change the base of support: wide--narrow.
-
Add movements of the head and/or eyes.
-
Challenge the visual system: close eyes.

-
Decrease the level of assistive device used: parallel bars, cane, no device.
-
Make the walking surface less stable, change the angles of surfaces.
-
Add obstacles, distractions, objects to carry or manipulate.
-
Increase the speed of walking.
-
Add manual resistance.
-
Add sudden directional changes.
-
Add movements of the head and/or eyes.
-
Challenge the visual system: dimly lit hallway.

Agility and reaction time exercises involve the ability to explosively start, decelerate, change direction, and accelerate again quickly while maintaining body control. These fast-paced exercises are the basic elements of technical skills. They cover the spectrum from dynamic gross activities to fine motor control activities and motor coordination.
Agility exercises are often referred to as drills, examples include:
-
Lateral Plyometric Jumps - Jumps side to side.
-
Tuck Jumps - Jumping straight up from a squat position, remaining tucked at the top of the jump before extending the legs to land.
-
Shuttle Runs - Sprinting from marker to marker with frequent changes in direction.
-
Forward-backward Sprints - Sprint forward to a cone, then jog backward to the start.
-
Speed Ladder Agility Drills - Using a type of sporting equipment that resembles a rope ladder, drills are done by running forward with high knees or running laterally.
-
Dot Drills - Jumping from dot to dot with both feet in an X shaped pattern.
The video below demonstrates a range of agility drills using a ladder formation. As can be seen, the swift movements require a high degree of neuromuscular coordination. However, there are some safety risks due to these rapid-fire movements, such as injuring the knee or ankle by twisting/straining it. Ensure proper form/posture is maintained and gradually build intensity (speed) as skill is developed.
Agility exercises should be undertaken regularly throughout the week. Progression is achieved by adding multiple phases that allow the client to gradually increase the level of difficulty. Phases last for approximately two weeks although this may vary from client to client. Difficulty is increased through the use of direction changes, longer durations, increased distance, greater speed required, and added resistance.
Plyometric training can improve power (including strength and speed). This type of exercise involves a short burst of energy to undertake a specific movement. Strength is used to achieve explosive movement and speed (reaction time) is used to rapidly commence and perform the movement.
Examples include squats, jumping, stair climbing, and push-ups. This method of training is often high-impact and can negatively affect joints. Of particular concern are the hips and knees.
Some tips for avoiding injury include:
-
Warm up - Never start exercising with plyometric activities, always undertake a light cardiovascular warm-up and stretching routine first.
-
Avoid hard surfaces - Consider outdoor grassed areas or indoor areas with appropriate floor padding.
-
Wear appropriate footwear - Cushioning is required.
-
Avoid overexertion - Stop if the client feels any pain, discomfort, or dizziness.
-
Gradually build intensity - Start with easier low-impact exercises and gradually increase the difficulty level and/or added weight.
Elite athletes may also use ballistic stretching exercises in which the body or an individual limb is moved beyond its normal range of motion and repeating this movement in a bouncing or jerking movement (ie. repeatedly bending down to touch toes). NOTE: This type of stretching is NOT recommended for inexperienced clients as it can cause injury.
Stretching muscles which can help prevent injury and/or discomfort by allowing lactic acid buildup to subside and easing tense muscles. Types of flexibility exercise include:
-
Ballistic - Moving the body or an individual limb beyond its normal range of motion and repeating this movement in a bouncing or jerking movement (ie. repeatedly bending down to touch toes). NOTE: This type of stretching is NOT recommended for inexperienced clients as it can cause injury.
-
Dynamic - Gradually stretching parts of the body to increase reach and/or speed. Uses controlled, gentle movements (ie. leg swings, arms swings or torso twists).
-
Static (Active) - Assuming a certain position and holding it with no assistance other than muscle strength (ie. isometric exercises like plank and some yoga poses like chair or tree).
-
Static (Passive) - Assuming a certain position and holding it with the assistance of another part of your body or a training partner or a form of apparatus (ie. bringing the leg up high and stretching it against a wall).
Dynamic stretching is normally recommended before a workout. This is because they are designed to keep the body moving, aiding in the warm-up process without tiring the muscles because the stretch is not held for long. They are especially good for athletes who are about to perform fast-burst activities such as sprinters or weight-lifters as this type of stretching helps to improve speed, agility, and acceleration.
Static stretching (either active or passive) is better after a workout. This is because static stretching contributes to muscle fatigue and muscle fibre damage and can reduce performance if done prior to physical activity. Static stretching helps to improve flexibility, achieve a wider range of motion of the joints, and reduce muscle soreness. Stretching is not recommended in the case of acute muscle soreness as this may increase damage.
An advanced form of flexibility training utilises a technique known as Proprioceptive Neuromuscular Facilitation (PNF) stretching. Often used as forms of rehabilitation it involves both stretching and contracting a muscle group.
To perform a PNF stretch the following steps should be followed:
-
Position the targetted muscle or muscle group into a state of stretch (tension).
-
Whilst the muscle is held in place by an immovable object (can be another person) contract the stretched muscle for 5-6 seconds.
-
Relax the contracted muscle and maintain the controlled stretch for another 20-30 seconds.
-
Allow a recovery period of 30 seconds before repeating the process (approximately 2-4 reps).
.jpg)
There are many benefits of exercise, both physical and mental. From a functional movement perspective, there are some key physiological adaptations (changes) that occur as a result of regular exercising.
These adaptations tend to affect the musculoskeletal and cardiorespiratory systems the most, however as both of these hybrid systems work in conjunction with the nervous system there are adaptations that are apparent with the central and peripheral nervous system.
Adaptations may be either short-term (acute) or long-term (chronic). Short-term adaptations can occur after a single bout of exercise and may include temporary and expected changes, such as muscle soreness, as well as unexpected incidents such as injuries. Long-term adaptations are the result of sustained exercise programs and usually include beneficial changes to a person's well-being and body composition, however, may also include the creation or exacerbation of a chronic injury if the physical activity is not properly executed or supervised.
The major physiological adaptations are:
These cardiac adaptations are closely linked to each other:
-
Resting heart rate - The number of beats per minute that the heart completes whilst at rest.
-
Stroke volume - The volume of blood ejected from the left ventricle of the heart during each beat.
-
Cardiac output - The volume of blood ejected from the heart per minute.
The short-term effects of exercise on cardiac performance include:
-
Increased heart rate - The heart begins to beat harder and faster to circulate blood and deliver oxygen and nutrients to muscles allowing them to function.
-
Increased blood pressure - As the heart rate becomes faster the systolic blood pressure rises. It is normal for systolic blood pressure to rise between 160 and 220 mm Hg, however, some clients may experience extreme rises which may cause health implications.
The long-term effects of exercise on cardiac performance include:
-
Improved heart muscle - The myocardium (middle and thickest layer of the heart wall) becomes thicker which results in a more forceful contraction (systole) and more efficient emptying of the left ventricle during the relaxation of the heart muscle (diastole).
-
Reduced heart rate - As the cardiovascular system improves the heart is able to pump more blood per beat and thus is able to have fewer beats per minute.
-
Reduced blood pressure - A more efficient heart that is beating less whilst still able to perform at the same level means that the force on the arteries is reduced and thus blood pressure will not rise as significantly during exercise.
Located in the red blood cells, haemoglobin binds to oxygen and transports it to the muscles. As a result of regular exercise, overall blood volume, blood plasma, and red blood cells increase which in turn increases haemoglobin levels.
As a result of this adaptation, a great amount of oxygen is delivered to the muscles during exercise.
The amount of oxygen used by muscles as they are working. Regular exercise helps to improve the oxygen delivery system of the body via the cardiovascular/circulatory system and thus VO2 Max levels are improved.
Lung capacity is the amount of air that the lungs are capable of inhaling with each breath. Regardless of whether an individual is physically fit or not they are capable of increasing their lung capacity if required. This is essentially what happens when someone takes a deep breath.
There actually isn't much difference between lung capacity limits of an athlete vs. an untrained individual, however, the overall strength of the lung muscles and surrounding tissue does improve which makes for more efficient ventilation. Regular exercise also increases the amount of capillaries which allows more volume of air to be absorbed.
The growth or improvement of muscle as a result of damage sustained to the fibres during resistance and endurance exercise. The subsequent repair process ads more myofibrils, myoglobin, mitochondria, and capillaries to the overall muscle increasing its size/power and/or its ability.
Motor units are the combination of motor neurons and skeletal muscle and are divided into three groups - type 1 (slow-twitch), and types 2A (intermediate fast-twitch) & 2B (fast-twitch). Fast-twitch muscle fibres are used by sprinters and weight lifters as they deliver powerful bursts of energy for short (2A) and very short (2B) durations. Slow-twitch fibres are used for endurance exercise like marathon running as they contain high levels of oxygen and nutrients to allow for sustained activity over long durations.
The short-term effects of exercise on muscle performance include:
-
Increased muscle temperature - Muscles experience a process of temperature increase (warm-up) during physical activity.
-
Increased elasticity - Warmer muscles become more elastic (flexible) and are less prone to injury. Stretching exercises help to improve this process.
-
Muscle fatigue - Experienced when the muscle depletes its reserves of oxygen, nutrients, and chemical compounds required to generate the force to contract. Lactic acid build-up also contributes to muscle fatigue.
-
Delayed Onset Muscle Soreness (DOMS) - Sore, aching, painful muscles that is a normal phenomenon experienced after unfamiliar and/or intense exercise, especially eccentric exercises. Eccentric exercise is when the muscle stays contracted while lengthening (as opposed to concentric exercise where the muscle contracts while shortening). Eccentric contraction exercises (ie. the downward motion of squats, push-ups, pull-ups, and crunches) recruit fewer motor units to help repair damaged muscle fibres and thus the 'injury' (soreness) results. Prevention of DOMS can be achieved through the use of anti-inflammatory medications, massage, compression garments, rest, and supplements. However, it is a common and temporary condition which shouldn't need much intervention.
Motor units which are regularly exercised with progressive overload (increased weight and/or longer duration) being applied will result in the long-term neuromuscular adaptation of hypertrophy occurring. Hypertrophy can be either:
-
Sarcoplasmic Hypertrophy - Improves the slow-twitch/type 1 muscle fibres. Results in sarcoplasm being increased thus improving the oxygen and nutrient delivery system.
-
Myofibrillar Hypertrophy - Improves the fast-twitch/types 2A and 2B muscle fibres. Results in additional myofibrils being added to the muscle thus increasing its overall size and strength.
The benefits of these neuromuscular adaptations include:
-
Better endurance for long-duration activities such as marathon running.
-
Greater power and speed to improve the strength and reaction time required for fast-paced activities.
Bones and joints are subject to a condition known as bone loss which means calcium and other nutrients are reduced from the overall bone mass (known as low bone density). In its extreme form this condition is known as osteoporosis. People with low bone density are more prone to fractures.
Regular exercise, especially resistance training which builds muscle strength, can help to reduce the rate of bone loss. Exercise can also improve balance and coordination which helps to prevent falls which inturn reduces injuries such as fractures.
Other physiological adaptations that may occur during exercise can be related to or influenced by environmental conditions:
Exercising in high-temperature and/or humid environments can cause the body to suffer from heat stress. There are two forms of heat stress:
-
Heat stress that is able to be compensated through dissipation. The body produces sweat and also distributes blood closer to the skin surface as a means of cooling itself.
-
Non-compensable heat stress. The first option is only applicable if the temperature and accompanying exercise remain within a reasonable range and the body can produce enough sweat and/or distribute blood rapidly enough. If not, the body cannot perform properly, dehydration sets in and physical ramifications start occurring such as dizziness, fatigue, weak pulse, muscle cramps, and nausea/vomiting.
Preventative measures to protect against harm when exercising in hot environments include reducing intensity, replenishing fluids and also passively resting if required. Also wearing appropriate clothing, ideally light-weight breathable fabrics.
Exercising in cold-temperature environments can also cause the body to suffer stress. The body attempts to regulate its temperature through the constriction and dilation of blood vessels so that minimal amounts of heat are lost. It also increases heat production by developing muscle tremors (shivering). These adaptions can have an adverse effect on the body, in particular the muscles, if sustained for too long. Some of the effects are:
-
Decreased muscle metabolism.
-
Decreased oxygen intake.
-
Decreased blood flow to the muscles.
Frostbite is a risk when exercising in the cold. Caused by exposing skin to freezing conditions it commonly occurs on the hands (fingers), feet (toes) and also the face (cheeks, ears and nose). Early signs include numbness, loss of feeling and stinging sensations. Ensure that extremities are well covered prior to exercise and if frostbite is suspected then immediately move indoors and seek medical assistance.
When cold temperatures are combined with extreme wind a phenomenon known as wind-chill factor becomes a risk. Wind can penetrate clothing and remove the insulating layer of warm air that surrounds the body. Wind also stirs up dust and dirt particles which can be inhaled or cause damage to eyes.
If the body also becomes wet during cold temperatures then the risk of hypothermia is greatly increased, emergency medical assistance may be required. Symptoms of hypothermia include:
-
Intense shivering.
-
Slurred speech.
-
Loss of coordination.
-
Fatigue.
Preventative measures to protect against harm when exercising in cold environments include wearing layers of appropriate clothing, wearing protective eye-wear, eating carbohydrates and replenishing fluids.
When exercising in the high altitude environments the body will not have access to the same oxygen levels than it does at sea level. This will affect endurance style exercises which require oxygen as an energy source.
It isn't so much that there is a lack of oxygen (even at 10,000 feet there is still enough oxygen available for the body's needs) it is the fact that the barometric pressure is less and thus oxygen is not forced into the body (and thus the bloodstream) as easily during the breathing process.
Over time the body can adapt to these environments by developing more red blood cells to help ease the struggle of getting oxygen. However, this method takes time and therefore care must be taken to allow adequate training and preparation prior to attempting exercise in high altitude environments.
Preventative measures to protect against harm when exercising at high altitude include gradual increases in intensity focussing on aerobic training, practicising yoga breathing rhythms (taking deep abdominal breaths), and drinking plenty of water.
Methods to measure exercise intensity include:
This approach requires having the ability to measure the client's heart rate periodically as they exercise and keeping it within their target heart rate zone.
-
Calculate the maximum heart rate. This number is related to a client's age. To estimate this number subtract their age from the number 220.
-
Find their target heart rate zone. This is a range at which the heart rate should remain while exercising.
For the frail, elderly and beginners, strive for 40 to 60% of their maximum heart rate. For healthy individuals, strive for 50 to 75% of their maximum heart rate. As a client increases their fitness level, their resting heart rate should drop and they will be able to work harder or longer while remaining in their target heart rate zone (which could be 60 to 85% of their MHR).
Finding Client’s Target Heart Rate
|
|
For the client |
Example |
|
AGE |
I'm ___ years old. |
50 |
|
MAXIMUM HEART RATE (MHR) |
220 minus my age equals ___. This is my maximum heart rate. |
220 – 50 = 170 |
|
MODERATE ACTIVITY |
My maximum heart rate of ___ x 0.60 = ___ beats per minute (bpm). My maximum heart rate of ___ x 0.70 = ___ bpm. My moderate level target heart rate is ___ to ___ bpm. |
The 60% level is 170 x 0.60. This is 102 beats per minute (bpm). The 70% level is 170 x 0.70. This is 119 bpm. The target heart rate is 102 to 119 bpm. |
|
VIGOROUS ACTIVITY |
My maximum heart rate of ___ x 0.70 = ___bpm. My maximum heart rate of ___ x 0.80 = ___ bpm. My vigorous level target heart rate is ___ to ___ bpm. |
The 70% level is 170 x 0.70. This is 119 bpm. The 80% level is 170 x 0.80. This is 136 bpm. The target heart rate is 119 to 136 bpm. |

Heart rate can be monitored manually or digitally:
-
Manual - Measure the heart rate either on the wrist (radial artery), at the base of the thumb (palm side) or at the side of the neck (carotid artery). Use two fingers and lightly press on the artery. A pulse beat can easily be felt. Count the number of beats in a 6-second period. Multiply this number by 10 to determine beats per minute. For example, if a 6-second count were 9, then the heart rate would be 90 beats per minute. Monitor heart rate periodically, while exercising, for best results.
-
Digitally - Heart rate is measured via a wearable device, ideally attached via a strap to the chest/sternum area.
The respiration rate is the rate or speed at which breaths are taken. A standard respiration rate for a resting adult is 14 breaths and this can increase to 36 breaths per minute as a result of exercise.
The rating of perceived exertion is a widely used and reliable indicator to monitor and guide exercise intensity. This approach requires rating a client's level of exertion during exercise. There are a few scales for measuring the rate of perceived exertion, namely the Borg Scale (has rating levels 6 - 20), and the Modified RPE scale (has rating levels 0 - 10). They are explained here.
The talk-test method is a simplified version of the RPE test. Essentially it determines that if a client can talk and exercise at the same time, they are NOT working too hard. This means that their oxygen needs are still being met. If the client is out of breath, they are probably working too hard (especially if they have to stop and catch their breath). The benefits of the 'talk test' is that it is quick and simple to conduct and requires no equipment but this test is limited in the fact that it is not exact. Different clients will be able to talk more or less during different levels of activity.
RPE scale of perceived exertion can be used to measure levels of exertion by placing the client on the tool below:
| Rating | Activity Level | Breathing and Conversation Ability |
|---|---|---|
| 0 | No Activity (Laying on the couch). | Breathing normal resting rate. |
| 1 | Very Light Activity (Easy chores such as washing the dishes). | Breathing not changed. Easy to carry on a conversation. |
| 2-3 | Light Activity (Leisurely walking that does not increase the heart rate). | Easy to breathe and carry on a conversation. |
| 4-6 | Moderate Activity (Brisk walking that speeds up the heart rate). | Breathing more heavily - can carry on a conversation but it requires more effort. |
| 7-8 | Vigorous Activity (Jogging, cycling, swimming). | On the verge on becoming uncomfortable - conversation requires maximum effort. |
| 9 | Very Hard Activity (Running). | Difficult to maintain exercise or speak. |
| 10 | Maximum Effort Activity (Short burst of activity such as a short sprint, cannot be maintained for long). | Full out effort - no conversation possible. |
A method of determining the technique, progression and intensity of a particular session is to count the number of sets and repetitions in order to determine the level of intensity that the client should be feeling at a particular stage of the session and modifying the session accordingly. It is also important to keep track of the amount of weight the client is lifting throughout the session.
A method of determining the technique, progression and intensity of a particular session is to count the number of sets and repetitions in order to determine the level of intensity that the client should be feeling at a particular stage of the session and modifying the session accordingly.
It is important to keep track of the amount of weight the client is lifting throughout the session.
Observing the client throughout the exercise is an excellent method of determining the technique, progression and intensity of an exercise. Look for signs of:
-
Consistency of movement.
-
Level of difficulty performing the movement.
-
Signs of fatigue.
-
Signs that the exercise is getting easier.
Prior to implementing an exercise plan it is recommended that a Functional Movement Screen (FMS) be conducted to ascertain abilities and limitations the client may have in regards to essential movement patterns with the view to avoiding injuries.
The functional movement screen is a series of seven movement patterns (based on, but not exactly the same as the seven functional movements) that require balance of mobility and stability exercises to be undertaken and assessed.
Each movement is scored from 0 to 3:
-
0 = Pain during movement.
-
1 = Failed movement pattern.
-
2 = Passed but with some compensations.
-
3 = Passed with no compensations.
A score of 1 means that movement should not be trained, but should be corrected. A score of 0 requires an evaluation performed by a competent medical professional. An asymmetry such as a score of 1 on one side and a 2 on the other points to an important movement dysfunction to correct. A total score of <=14 on the FMS is used as the cut-off score, individuals who score less than 14 are at greater risk of injury.
FMS identifies those exercises considered most effective to restore proper movement patterns and to build strength.
Information on correction of asymmetries and further FMS research can be sourced from a variety of authoritative avenues:
-
Industry associations
-
Websites (for example, Runner’s World).
-
Health and Fitness Articles (for example, Men’s Health).
-
Medical journals (for example, collegiate strength and conditioning journals).
-
Seminars and courses on movement patterns.
-
Literature review.
