Micronutrients are nutrients which are needed in small amounts but can play a large role in a well-functioning body. Micronutrients play a central part in metabolism and in the maintenance of tissue function. Those who become deficient in micronutrients can suffer complications ranging from mild to severe.
The MoH Guidelines are designed to provide adequate intake of key micronutrients, but as our earlier discussions have highlighted, on average the NZ population is not consuming adequate amounts of key micronutrient rich foods weekly (especially fruit and vegetables). Ensuring adequate intake of micronutrients is therefore necessary and many people have turned to supplementation to try to make up for inadequate dietary intake. Supplements often contain super doses of these micronutrients and research is emerging that provision of excess supplements to people who do not need them may be harmful (Shenkin, 2006).
Within this topic we will explore the role of key micronutrients as they relate to athletic performance (and health). You will gain in-depth knowledge of the following:
- Historical micronutrient deficiencies in the New Zealand Population and whether they remain valid concerns.
- The extent of dietary supplement consumption in New Zealand
- Benefits and risks of supplement use
- The effectiveness of dietary supplementation - can it replace the real thing (food)?
- Micronutrients considerations for athletic performance
- Supplementation for performance enhancement – a look at widely used supplements and the research supporting their use
- Regulation of dietary supplements in NZ
- Referral pathways for clients seeking advice on supplementation
- Other foods and supplements that may enhance performance – a close look at “functional nutrients” and the research behind them.
While it falls outside the PT scope of practice to recommend any health or performance enhancement supplement to our clients, it is important you have a broad understanding of the supplements that are commonly used by regular clients and athletic populations, so you are able to answer client questions. It is also important that you know who to refer clients to, should they need further assistance.
Terminology
Become familiar with the key terms and measurement units that will serve as the building blocks for comprehending the intricacies of various micronutrients, dietary supplements, and the role of food in promoting health. By familiarsing yourself with these concepts early on, you'll be better equipped to dive into the nuanced discussions and recommendations surrounding the use of micronutrients and supplements as medicinal tools.
| Term | Definition |
|---|---|
| Vitamin | Organic substances that are required in small quantities for normal health and growth |
| Mineral | Inorganic substances needed in small amounts to support normal bodily functions |
| Gram | 1 thousandth of a kilogram. There are 4.2g in a tsp of sugar |
| Milligram (mg) | 1 thousandth of a gram. Take a quarter of a tsp of sugar and divide that by 1000. |
| Microgram (mcg or µg) | 1 millionth of a gram, or one thousandth of a milligram (too small an amount to use the sugar example!) |
| Trace (amounts) | A minute and barely detectable amount of a substance |
| Recommended Daily Amount (RDA) | The amount of a nutrient that is considered adequate to consume daily for normal bodily functions |
There are a number of micronutrients that have been indicated as worthy of concern in NZ over the last few decades. Some of these proposed deficiencies are considered the result of inadequate diet, while others may have come about through intensive farming practices and reduced levels of key micronutrients in the soil in which food is grown. This has prompted worries of deficiency in the general public and prompted many New Zealanders to seek supplementation for fear of suffering health complaints. This section of learning will look at each of the “concerning” micronutrients in question, discuss whether the concerns are valid and identify the groups that may be at risk of deficiency.
The following information comes from a document written by Young and Mackay (2020) and published by Activity and Nutrition in Aotearoa. The data discussed in this report came from the Adult Nutrition Survey (2008/2009), the Total Diet Survey NZ (2016) and the NZ Health Survey (2014/2015).
Iron

Iron is essential throughout life, but needs are higher during periods of growth such as childhood, adolescence and during menstruation and pregnancy. Those following restricted diets like vegetarians and vegans may also be at higher risk of deficiency.
Iron deficiency from low iron intake, blood loss or increased demand (e.g. athletes) for an extended period can lead to iron deficiency anaemia which can impair immune function, increase tiredness, and affect cognitive function. Iron is absorbed more readily from animal foods (meat, chicken, fish) although absorption from plant-based sources is enhanced by eating meat, fish or chicken with vitamin C-containing foods. Interestingly absorption of iron has been shown to be inhibited by tannins in tea and phytates in wholegrain cereals
Iron deficiency in most instances appears to be linked to inadequate intake of iron-rich foods such as meat, chicken and fish, certain cereals, beans and lentils and dark leafy greens.
Groups at risk of low iron
The surveys that this data was extracted from suggest around 5-7% of the NZ population have low dietary iron intake. Women (9.7%) were more at risk than men (1.2%), especially Maori women (18.4%) and Pacifica women (19.9%).
Of particular concern were females aged 15-18 years (34.2%), with Māori females (49%) and Pacifica females (40%) even more at risk. Women aged 75+ years had the highest prevalence of iron deficiency anaemia (16.8%) followed by the 35-44 years age group (15.6%). Among men, the highest prevalence was shown in the 75+ years age group (27%).
Supplementation of iron
Iron supplements are readily available and should be considered by those identified as higher risk above, especially if it is difficult for them to maintain the required intake of iron-rich foods on a regular basis.
Calcium and Vitamin D

Adequate intake of calcium and Vitamin D is important throughout life to build and strengthen bones and to reduce bone loss. Low dietary intakes of calcium are associated with bone loss over the life course, resulting in a greater risk of osteoporosis. Bone mass or density tends to reduce with age, particularly after menopause in women. Older people are at risk of developing osteoporosis as calcium absorption decreases with age.
Low bone density increases the likelihood of fractures. The burden of fractures from osteoporosis in New Zealand increased by 37% between 2007 and 2020 showing this is a growing issue. Although calcium intake over the life course is a major factor affecting the prevalence of osteoporosis, other factors play a role, including Vitamin D status and physical activity.
Excessive protein intake, sodium and caffeine intake can also adversely affect calcium status by increasing calcium loss from the body. Older people may be put at further risk due to reduced absorption of calcium through insufficient gut secretions in older adults.
Vitamin D status is predominantly maintained by exposure to sunlight as dietary sources are thought to only provide small amounts of Vitamin D. Preventative strategies include ensuring adequate calcium and Vitamin D intakes and weight-bearing exercise as well as fracture prevention.
Low calcium intake is most likely the result of insufficient intake of calcium-rich foods such as milk and dairy products, nuts and leafy green vegetables. while Vitamin D deficiency is likely a combination of inadequate dietary intake along with lack of exposure to daylight.
Groups at risk of low calcium
The estimated prevalence of inadequate calcium intake in NZ intake is around 60% (women 73%, men 45%), and is higher (more than 90%) among Māori and Pacific women aged 15-18 years and 51+ years. The calcium intake of older people (>70 years) in particular is well below the Recommended Dietary Intake of 1300mg/day with survey results suggesting those aged 65-74 years, have usual daily intakes of only 684mg calcium per day for women and 844mg per day for men.
Groups at risk of low vitamin D
The surveys suggest most adults (68%) had adequate levels of Vitamin D with only 5% of adults found to be Vitamin D deficient (although one in four were below the recommended intake levels but not yet deficient). The prevalence of Vitamin D deficiency does not affect a particular gender or age group, but Pacific adults were 2.4 times more likely to be deficient than non-pacific.
Dietary supplementation with calcium and vitamin D
This is only recommended for people at high risk of a low calcium and Vitamin D status. Deficiency is easily rectified by consumption of calcium-rich foods, but those who are lactate intolerant, or choose not to eat animal products may benefit from supplementation.
Iodine

Iodine has long been a micronutrient of concern in NZ as our soil content of iodine is low. This means foods that are grown in these soils will be inadequate sources of iodine which predisposes the NZ population to lower intakes.
Iodine is an integral part of the thyroid hormone responsible for normal growth and development of the body including the brain, and processes controlling the body’s metabolic rate. Iodine deficiency affects normal brain development.
It appears that Government-level fortification initiatives have been successful in increasing the iodine consumption of the general NZ population. Salt has been iodised in New Zealand since the 1920s as a public health measure to reduce health issues that were presented at that time. Widespread monitoring of iodine deficiency carried out in the 1990s showed that mild iodine deficiency was present in some population groups including children. In response to this declining intake of iodine, mandatory fortification of bread with iodised salt was introduced in 2009.
Groups at risk of low iodine
Almost no one at present. More recent surveys indicate that iodine was adequate across most population demographics, however, women of European/Other ethnicities reported mild iodine deficiency. The Total Diet Survey (2016) showed that fortification of bread with iodine and other food sources of iodine provided sufficient intake of iodine in the New Zealand diet.
Supplementation with iodine
Appears largely unnecessary if bread and iodised salt are consumed daily. Studies have shown that pregnant women require more iodine and may benefit from supplementation. This led to the NZ Government recommending and subsidising an iodine supplement for pregnant and breastfeeding women back in 2010.
Selenium

Selenium is an essential trace element in the diet; however, New Zealand soils are naturally low in selenium and hence the New Zealand food supply contains low levels. However, our low selenium intake compared to international intakes, has not been associated with any adverse health conditions.
Although concentrations in New Zealand soils are low, there is no indication that this has resulted in any detrimental effects on the health of New Zealanders. This is mainly due to the consumption of imported plant foods including Australian wheat which is high in selenium.
Internationally, there is low-level evidence that low blood levels of selenium may increase the risk of prostate cancer.
Groups at risk of low selenium
While our current intake of selenium are lower than in other countries, the New Zealand diet appears to contain adequate amounts of dietary selenium to provide for the nutritional needs of the population. In the 2008/09 survey, 45% of the adult population was estimated to have an inadequate intake of selenium. Older people (71+ years) and females aged 15-18 years were the age groups most likely to have low intakes along with breastfeeding and post-menopausal women.
Supplementation with selenium
While our national intakes of selenium aren’t keeping up with those of other countries, there doesn’t appear to be a significant concern among our experts. Selenium intakes can be enhanced through consuming foods like organ meats (e.g. liver), yoghurt, seafood, Brazil nuts, grains and cereals.
Zinc

Zinc is involved in many body processes. Deficiency results in impaired growth, wound healing, and immune system functioning. The 2008/09 survey suggested a quarter of the adult population had a lower-than-recommended zinc intake (24.7%). Low intakes of zinc are due to inadequate dietary intakes of zinc-rich foods such as seafood (especially shellfish), animal products, cashews, peanuts, and almonds.
Groups at risk of low zinc
A 2011 review of zinc status in Australia and New Zealand showed that groups of concern were toddlers, adolescents (in particular, the Pacific), and older people. Older males and females (71+ years) appear to have the lowest zinc intakes.
During pregnancy and breastfeeding, there is an increased requirement for zinc. Also, people on vegetarian or vegan diets may need higher intakes to allow for lower absorption of zinc from plant-based sources.
Supplementation with zinc
Those that fit into the higher-risk demographics may benefit from zinc supplementation, especially older populations and active adolescents.
Vitamin B12

Vitamin B12 is an essential vitamin for a wide range of functions in the body including metabolism, the nervous system, DNA synthesis and the production of red blood cells. Deficiency results in a specific type of anaemia and neurological dysfunction.
The 2008/09 suggests that approximately 8% of the population had a low intake.
Groups at risk of low B12
Young women (19-30 years) had the highest prevalence of low intake (about 23%) and 30% of a sample of young women surveyed in 2014/15 had intakes below the Estimated Average Requirement (EAR). Around a quarter of participants 85+ age group (26% Māori, 22% non-Māori) had an intake less than the EAR for Vitamin B12.
Vitamin B12 is predominantly found in animal products, so those who follow meat or animal-free diets may be more at risk of a Vitamin B12 deficiency. The prevalence of vegetarian or vegan diets in NZ is unknown but has grown substantially since these surveys, which suggests the rates of B12 deficiency may have increased somewhat.
Supplementation with B12
It seems pretty clear that young women (particularly those following restrictive dietary practices, along with older population members, may benefit from B12 supplementation.
It appears that concerns over deficiencies in these particular nutrients do not apply to the entire population. Men, in general, seem to meet the dietary requirements for most of these nutrients. However, New Zealand women, especially adolescents, non-European individuals, and older adults, are at considerable risk for inadequate intake of these key micronutrients. Considering that we are an aging population, this must be a significant focus in the future, as the potential stress on our healthcare system could be significant. Changes in gut function among older populations mean they struggle to absorb the same amount of nutrients from their diet as younger groups. This necessitates them to consume even more nutrient-rich foods, which can be challenging given that appetite and energy expenditure rates tend to decrease with age. Therefore, supplementation may be a viable and necessary option for our older populations.
National nutrition surveys in NZ are very infrequent, with the last full survey completed in 2008/2009. This means finding up-to-date information on supplement use in NZ is difficult to qualify as most recent surveys or research articles focus on small samples or specific sectors of the community. Here is what the available literature tells us about supplement use in New Zealand over recent years.
The 2008/2009 New Zealand Adult Nutrition Survey reported that:
- 46.7% of all NZ adults aged 15 and over had used a dietary supplement in the last year (females 53%, males 42%). 30% of these supplement users were regular (daily or weekly) users.
- Females tended to consume more supplements than males at any age and supplement use appeared to peak between 31-50 years of age in females and 71+ years in males.
- The most frequently consumed supplements were:
- Oils (e.g. fish and plant oil) - 16%
- Multi-vitamins/minerals - 15%
- Herbal supplements – 10%
- Single vitamins – 9%
- Botanicals like plant extracts – 8.5%
- Glucosamine/chondroitin (for joints) - 6.2%
More recent information suggests that we consume more dietary supplements than ever before. Retail sales of non-prescribed supplements are reported to have increased in New Zealand by 74% between 2007 and 2021 (McLeod et al, 2022). These authors suggest that supplement sales have risen from $194 million to $335.5 million annually over this period.
An article published in the NZ Herald titled “Kiwis Pay a High Price For Health” (2019) suggests that those figures are very conservative and that the true figure that NZ people spend on supplements is closer to a billion dollars a year with vitamin and mineral supplements making up the majority of sales. The largest chunk of these sales seems to be for vitamin C and D supplements in response to media reports that they may be useful in warding off COVID. There is no scientific evidence to support this.
Within this article, leading NZ Nutritionist Sarah Hanrahan says this may be to make up for the fact that most New Zealanders don’t meet their daily recommendation of fruit, vegetables or whole foods. Hanrahan went on to say that while supplements can be beneficial for people at certain ages or with particular dietary needs, real food is a much better (and cheaper) way to get your micronutrient needs.
A 2015 Southern Cross Healthcare Survey suggested that 1.5 million New Zealanders regularly take dietary supplements, and many spend more than $50 a month to do so. The survey suggested that around half of these supplement users had used them habitually for years.
Supplement Usage Study by McLeod et al (2022)
McLeod et al conducted research on a cohort of 1,265 Christchurch residents, part of a long-term health and development study since their birth in 1977. Here are key findings from their report:
- Supplement usage
- 36% of the surveyed group reported using supplements.
- Gender differences
- Females (61.4%) were more likely to take supplements than males (38.6%).
- Number of supplements
- The highest number of supplements taken by individuals in the study were nine for females and seven for males.
- Types of supplements
- A total of 626 different supplement products were consumed.
- Most common categories included vitamins and minerals (61%), probiotics, Q10, and bee products (12.5%), and oils and herbal botanicals (9.6% each).
- Supplements without scientific evidence
- 12% of those surveyed used products with no scientific evidence.
- Common examples: are turmeric/curcumin for IBS and joints, evening primrose oil for anti-inflammatory purposes, and spirulina for gut health.
- Supplements for non-evidence-based reasons
- An additional 30% used supplements for reasons not supported by evidence.
- Common examples: are magnesium for sleep, fish oils for allergies, and vitamin C for immunity.
- Excessive dose consumption
- 11% of supplement users were taking potentially excessive doses.
- Negative interactions
- 10 of the supplement users in the survey experienced potential negative interactions.
- These interactions were often considered "moderately severe" and linked to other prescribed medications.
Finally, Consumer NZ conducted their own survey on 1001 people in 2022 and reported that 80% of the people they surveyed had taken a supplement in the last year with multivitamins (55%) and vitamins (54%) the most popular choice (Thian, 2023).
Reasons for supplement usage in new zealand
What is obvious from the survey data above is that supplements are popular in NZ! But why are people taking them?
When Consumer NZ asked 1001 Kiwis why they were taking supplements, these were the most common responses:
- Perceived vitamin or mineral deficiencies (31%)
- Joint health/pain (27%)
- Sleep improvement (24%)
- Energy improvement (23%)
- Immunity (23%)
- Gut health (20%)
- Mental health or anxiety (19%).
The following list shows the percentage of people surveyed with the top four main reasons why they took supplements. Flick through each reason and flip each card to reveal the percentage.
Despite the apparent high use of supplements in NZ, only 33% of those surveyed had done any of their own research on the evidence-based effectiveness of the supplement they were taking. Of these people, more than half (59%) used the internet with the others seeking advice from a pharmacist (28%), friends and family (23%) and a GP (21%).
Over 50% of the surveyed people had no idea if the supplement they were taking actually worked and almost none of them had been prescribed the supplement they were taking by a health professional (although 11% took them because a doctor had recommended them). 49% had purchased the supplement from a supermarket, while 47% had purchased theirs at a pharmacy (Thian, 2023).
35% of those surveyed believed that supplements were not necessary if they ate a balanced diet. 22% disagreed with this statement (43% were unsure).
Image source: https://www.consumer.org.nz/articles/why-are-natural-health-products-so-popular
When Consumer NZ (2022) asked if they were at all concerned about the safety, effectiveness, ingredients and quality of the dietary supplements and natural remedies they were taking about half the respondents in the survey said they were “somewhat, very or extremely concerned”. A similar number said they are concerned about the health effects of long-term use and the risks of taking them with prescription and non-prescription medicines.
This means that despite the regular consumption of supplements, over half of these people had concerns about the risks associated with taking them.
When asked whether they thought there were serious issues that could arise from taking too much natural remedy or supplement, 25% of those surveyed did not think this was possible, while 51% were aware this could happen (24% were unsure). The majority (73%) believed that supplements were safe to use if consumed as recommended on the label and 63% were aware that supplements might interfere with prescription medications (Consumer NZ, 2022).
The information collected from the surveys and articles above raises some interesting questions about supplements:
- Do dietary supplements deliver the benefits they promise?
- Can they adequately substitute real food or compensate for a subpar diet?
- What are the potential risks of excessive dietary supplement intake?
The effectiveness of supplement intake
This is a contentious area of debate. There is support for the use of supplements in certain populations where obtaining everything they need from food becomes difficult. These groups include but are not limited to:
- Older populations with reduced gut absorption abilities.
- Those that consume restrictive diets – e.g. non-meat eaters.
- Pregnant or breast-feeding women.
- Those with diagnosed medical conditions- such as anemia.
But what about people who consume a relatively balanced diet? Is there a benefit to adding supplements to the diet? With the amount of money being spent on dietary supplements in New Zealand it seems fair to assume that the majority are being bought by those who can afford them. University of Otago Professor Jim Mann suggests that those who buy supplements are “basically the rich folks, who are worried about their health...” This suggests that many of the people who can afford to buy supplements don’t need them. This is supported by the fact that those who are commonly reported as deficient in micronutrients are from the lower socioeconomic areas of our communities. Those who typically buy supplements tend to be more health conscious and can afford better daily dietary intakes.
There are suggestions that consuming additional supplements thinking this will offer additional benefit may be a waste of money. Guallar, Stranges and Mulrow (2013) performed a systematic review of the existing evidence related to vitamin and mineral supplements and concluded that “Enough is enough: Stop wasting money on vitamin and mineral supplements.”
Research on Supplements: What the Studies Show
- All-cause mortality and chronic diseases
- Comprehensive trials with over 400,000 subjects found no clear evidence of supplements benefiting all-cause mortality, cardiovascular disease, or cancer in adults without nutritional deficiencies.
- Cognitive performance in older adults
- A study on 5947 older adults using daily multivitamins showed no impact on cognitive performance over 12 years.
- A review of 12 studies on vitamins B, C, E, and fish oil found no cognitive improvement in individuals with mild to moderate dementia.
- Cardiovascular health
- A study involving 1708 individuals who had experienced heart attacks found no cardiovascular benefits from a high-dose 28-component multivitamin after 5 years.
- Chronic disease prevention
- Multiple reviews on vitamin and mineral supplementation for chronic disease prevention consistently showed null results or, even worse, potential harm.
- Studies on antioxidants, folic acid, B vitamins, and multivitamins have also reported no significant effects.
The overall conclusions of this systematic review could not have been stated more clearly:
“The message is simple: Most supplements do not prevent chronic disease or death, their use is not justified, and they should be avoided. This message is especially true for the general population who have not been diagnosed with a micronutrient deficiency (this represents most supplement users).”
(Guallar, Stranges and Mulrow (2013)
The following video supports these findings as it discusses some common myths associated with supplements.
Suitable recipients of supplements
The consensus of most health professionals is that adults who are not deficient in micronutrients will receive no benefit from taking additional supplements. That makes sense. But we have already discussed that a number of our population is not getting the required amounts of certain micronutrients. There is ample evidence to suggest that micronutrient supplementation can have an effect on those with increased needs, or that are deficient. Take a look at the following table to view examples of these benefits, (be mindful that they are not limited to only these listed in the table):
| Supplemental folic acid for pregnant women | Multiple studies from the 1990s and early 2000s found folic acid supplementation prevented neural tube defects in babies when women take it before and during early pregnancy. |
|---|---|
| Supplemental iron for diagnosed anaemia and low iron status in menstruating women | Low et al (2016) concluded that daily iron supplementation effectively reduces the prevalence of anaemia and iron deficiency, and raises hemoglobin levels and iron stores in menstruating women with low iron. Note: This effect often comes with gastrointestinal side effects. |
| Supplementation of E for cataracts and pre-e | A meta-analysis performed by Zhang et al (2015) concluded that supplementation of vitamin E was significantly correlated with a reduction in age-related cataract risk. |
| Calcium and Vitamin D supplementation to prevent osteoporosis in elderly | Has been shown to prevent or improve the condition of osteoporosis but may do so at a cost. A meta-analysis by Li et al (2022) found that calcium supplementation prevented osteoporosis and osteoporotic fractures but may also increase the risk of cardiovascular disease and kidney stones. |
These examples share a common theme. Those who experienced benefits from micronutrient supplementation were either elderly individuals, a group recognised for its deficiencies, or individuals with unique dietary needs. These cases fall beyond the scope of our practice when providing specific dietary recommendations.
Risks associated with unnecessary micronutrient supplementation
Supplementing micronutrient deficiencies can be beneficial, but taking unnecessary supplements can pose risks. While water-soluble micronutrients like vitamins B and C can be excreted in urine if consumed in excess, fat-soluble vitamins and other micronutrients may accumulate in the body to potentially harmful levels. For example, there is clear evidence from studies involving tens of thousands of people randomly assigned in clinical trials showing that excess intake of B-carotene (antioxidant), Vitamin E and possibly high doses of vitamin A supplements increase lung cancer and total mortality (Guallar, Stranges and Mulrow, 2013).
Click on the following commonly used vitamins and minerals to reveal their potential adverse effects.
Acute toxicity associated with ingestion >300,000 IU. Chronic toxicity (hypervitaminosis) associated with doses >10,000 IU/day. Symptoms of chronic hypervitaminosis A include skin desquamation, liver impairment, loss of vision and severe intracranial hypertension.
Moderate to high doses of vitamin B3 are commonly associated with peripheral vasodilation causing skin flushing, burning sensation, pruritus and hypotension. Vasodilation may also occur in the eye resulting in reversible toxic cystoid macular oedema.
Doses ≥200 mg/day of vitamin B6 have been associated with severe sensory peripheral neuropathies. Risk often arises from multiple products being taken all containing pyridoxine.
Associated with precipitation of cysteine, urate or oxalate kidney stones, especially in people with a predisposition for kidney stones. Vitamin C may reduce the effectiveness of antineoplastic drugs such as vincristine, doxorubicin, methotrexate, cisplatin and imatinib.
Very high doses may cause hypercalcaemia, with symptoms from thirst and polyuria to seizures, coma and death. High intermittent doses of vitamin D have been associated with increased risk of falls and fractures in the elderly.
Antiplatelet effect and increased risk of haemorrhagic stroke reported.
Carbonate salt can cause gastric reflux and constipation. High-dose calcium may induce vascular and soft tissue calcification, hypercalciuria, kidney stones and secondary hypoparathyroidism. Interferes with absorption of magnesium, iron and zinc if taken simultaneously, and can reduce the absorption of many other drugs e.g. levothyroxine, and tetracyclines.
High doses often result in diarrhoea, nausea and abdominal cramping due to the osmotic effect. Like other divalent cations, magnesium may chelate and reduce the absorption of other minerals or medicines such as tetracyclines.
Often associated with altered or impaired taste and smell. Intranasal zinc can cause anosmia. Doses ≥80 mg/day in clinical trials were associated with adverse prostate effects.
Associated with acute and chronic toxicity. Signs of chronic high-dose ‘selenosis’ are hair and nail loss or brittleness, lesions of the skin and nervous system, nausea, diarrhoea, skin rashes, mottled teeth, fatigue and mood irritability.
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8377299/
Brown (2016) suggests the following:
- Pregnant women need to be especially careful with their vitamin A intake, as excess amounts have been linked to birth defects.
- Results from many clinical trials show that beta-carotene, vitamin E, and possibly high doses of vitamin A can increase the risk of premature death.
- Other studies have linked multivitamin use to increased cancer risk, and iron supplements can be harmful for people who don’t need them.
- There is also some evidence that synthetic folic acid is more harmful than the natural folate in foods. It may build up in the body and raise the risk of cancer.
It is not necessary to go into these negative effects in detail. This information is provided simply to enlighten you that these seemingly harmless “health products” (that a good number of your clients will be taking) can have serious and potentially even life-threatening effects. They may cause these effects on their own, or in combination with other supplements or prescription medications. This is why it is important that personal trainers act within their scope of practice and refer clients that are considering taking supplements to an appropriate nutrition professional like a registered dietician who has in-depth knowledge of the effects supplements may have on medical conditions or prescribed medications.
Individuals adhering to a well-balanced diet are generally unlikely to experience micronutrient deficiencies, thus rendering supplementation unnecessary. The most effective preventive measure against deficiencies is to adhere to the Ministry of Health's Nutrition Guidelines and consume recommended servings from each food group.
However, specific populations, such as the elderly, individuals from lower socioeconomic backgrounds, those with restrictive diets, or certain medical conditions, may derive benefits from targeted supplementation. Such supplementation should only be initiated following a confirmed diagnosis by a qualified medical professional. Additionally, athletes with rigorous training regimens may have unique considerations.
Dietary supplements have a range of potential risks and few proven benefits. The following video sums up the benefits, risks and best approach for using dietary supplements.
Synthetic supplements vs. real food
The vast majority of health supplements are synthetic. This means that they have been made artificially in a lab or factory to mimic the way that naturally occurring micronutrients act in our bodies. To tell if a supplement is derived from natural or synthetic sources, check the label. Naturally derived supplements will usually list the food source they were derived from or will be labelled as “100% plant or animal-based”.
Why does it matter? For many years it was unclear how well synthetic nutrients were absorbed and used by the body (bioavailability). While it appears that some synthetic nutrients absorb better than others, recent studies indicate that absorption of most nutrients is similar between synthetic and natural sources although some small differences remain. Brown (2016) explains the likely reasons behind potential differences in the following way:
- When you eat real food, you are not usually consuming single nutrients, but rather a range of vitamins, minerals, co-factors and enzymes that allow for optimal absorption and use by the body.
- It is suggested that without the additional compounds, synthetic nutrients are unlikely to be absorbed and used a readily.
Click on the common supplements to reveal what the research proclaims:
Carr and Vissers (2013) compared the bioavailability of Vitamin C from synthetic and real food forms and found that there was no difference between synthetic and real food sources.
Lindschinger et al (2019) reported that despite favourable tendencies within the “natural” group, there were no statistically significant differences between the bioavailability of synthetic and real food sources of vitamin B.
There are two forms of vitamin D that we consume. Vitamin D3 is derived from animal products and Vitamin D2 is derived from plants. Most research indicates that Vitamin D3 has more of an effect on blood levels of Vitamin D suggesting it has a better absorption rate. Vitamin D2 is cheaper to produce synthetically, so is the most used form in supplementation. When choosing Vitamin D supplements, people should choose those containing Vitamin D3. These have been shown to have similar absorption rates to real food sources (Arnarson, 2023).
It appears real food sources are better than synthetic sources when it comes to vitamin E. The results of a study by Burton et al (1998) concluded that natural forms of Vitamin E yielded twice the availability of synthetic versions.
Schurgers et al (2007) suggest natural forms of vitamin K have 7-8 times the uptake of synthetic versions and have a longer and more pronounced effect. If buying a Vitamin K supplement, those containing the MK-7 natural source are preferred over synthetic K1 versions.
While calcium supplements appear to offer similar rates of absorption to food and milk products, they are best absorbed alongside food. There are many different types of calcium supplements, and some have negative side effects. The most commonly contain calcium carbonate, calcium phosphate or calcium citrate. Calcium carbonate is the least expensive version but often causes constipation and bloating. The others are more expensive but have fewer side effects (Garg and Mahalle, 2019). It appears that absorption of supplements is increased if taken alongside vitamin D. Many natural food sources of calcium also contain vitamin D which is why before supplementation is considered, a focus on getting the required amount of calcium from real food is preferred.
The absorption of iron supplements is on par with that of real food, however traditional ferrous iron-based supplements cause a number of gastrointestinal issues. Neto et al (2019) conducted a systematic review and meta-analysis on iron supplements versus real food and concluded that iron supplementation significantly increased haemoglobin levels in anaemic and iron-deficient subjects (even better than food consumption in some studies). Overall, there was little difference between the consumption of iron in food form or supplemented form.
Magnesium supplements can be absorbed at a rate comparable to real food sources. However, it's important to note that magnesium supplements come in various forms, such as magnesium oxide, citrate, and chloride, each with varying absorption rates. Magnesium forms that readily dissolve in liquids are absorbed more thoroughly in the gut compared to less soluble forms. Small studies have found that magnesium in the aspartate, citrate, lactate, and chloride forms is absorbed more completely and is more bioavailable than magnesium oxide and magnesium sulphate. Pardo et al (2021) suggest organic forms of magnesium are more bioavailable than inorganic forms. These authors concluded that all magnesium supplements can maintain appropriate levels of magnesium in those without a deficit, although this may not be the case for older people or those with illnesses.
Zinc supplements seem to mimic real food absorption rates and while there are a number of different Zinc supplement sources, none appear to be any better than others. Animal proteins appear to enhance zinc uptake which could suggest a benefit to real food consumption, however many other factors in real food sources like milk, iron, phytates (in cereals and soy) can inhibit zinc absorption (Smith, 2020).
Many synthetic supplement versions of common vitamins and minerals closely replicate the absorption and utilisation found in natural food sources. However, virtually all nutrition experts advise prioritising micronutrient intake from real foods whenever possible. Supplements are generally recommended for individuals who are unable to consume certain foods due to allergies or medical conditions, as well as those with impaired gut absorption, such as the elderly. The primary rationale behind this recommendation lies in the fact that excessive intake of micronutrients and its associated adverse health effects are challenging to achieve through whole foods but considerably easier through supplements. Additionally, concerns about the regulation and monitoring of micronutrient supplements in New Zealand further underscore the need for caution in their usage.
Supplement monitoring and regulation
Dietary supplements in NZ are regulated under the Dietary Supplement Regulations (1985), which fall under the Food Act, 2014 which is the responsibility of Medsafe NZ. Essentially, these regulations set limits for maximal daily intake doses, and labelling of a supplement and stipulate rules around the use of misleading statements and therapeutic claims (Dietary Supplements Regulations, 1985).
According to Wannan (2020), a product that doesn’t provide the nutrients or dose listed on the label would breach the supplementation regulations (and the Fair Trading Act) and could see the company that produced it hit with a $600,000 fine. However, the only way to test a supplement is via expensive testing procedures, so this is rarely done.
In terms of health or therapeutic claims, although supplement labels can’t claim to treat or prevent a condition, suppliers get around this by using vague language like “may assist”, “may help”, or “can support” (Wannan, 2020).
There is no pre-approval process for dietary supplements in NZ. The responsibility to ensure a supplement is made to an acceptable standard is safe to use and complies with the law falls on the manufacturer (Medsafe NZ, 2023).
While in other areas of the world like the EU, supplement manufacturers must submit evidence to the European Food Safety Authority and have a claim approved before putting it in advertising or on labels, there is no such pre-approval in NZ. During a quick check of supplements on a supermarket shelf Consumer NZ found multiple supplement products that recommended (or contained) amounts of a vitamin or mineral that were above the maximum doses stipulated by Dietary Supplements Regulations (1985).
There are also substantial concerns that a number of supplements do not contain what is stated on their label. In fact, dietary supplements are often mislabelled. A 2019 DILIN study checked the contents of herbal and dietary supplements collected from patients. Of 272 products, the chemical contents of half of them didn't match their label (Arnold, 2021), with some containing next to none of the micronutrients being marketed and others well above the level stated on the label.
So, it would appear that until a comprehensive regulatory system is adopted in NZ, a clear risk associated with supplements is that the reliability of what a supplement contains is highly questionable. This is likely why almost all nutrition professionals recommend we get our micronutrients from real foods wherever possible.
On a positive note, in 2022, the NZ Government introduced the Therapeutic Products Bill to parliament, which will regulate natural health products, among other things. Once this is passed it will more strictly regulate the ingredients that are allowed in supplements and the claims that can be made about the products. It will also contain a register of supplements which will be made publicly available, so consumers will be able to see the evidence associated with each product (Thian, 2023). Hopefully, this new Bill will improve the regulation of supplement products and lead to a greater level of assurance for consumers.
Try it out
Test your knowledge with the following set of questions.
Micronutrients play an important role in activity. While they are not direct sources of energy, they do facilitate energy production and utilisation from carbohydrates, fats, and proteins. They also allow the transport of oxygen and carbon dioxide, regulate fluid balance; and protect against oxidative damage.
Many of the B vitamins (thiamin, riboflavin, niacin, B6, and pantothenic acid) and some minerals (iron, magnesium, copper, and zinc) are needed for the metabolism of carbohydrates into energy for muscle work.
Iron, copper, B6, B12, and folate are required for red blood cell (RBC) formation and oxygen (O2) transport to muscle cells.
Zinc is essential for the removal of carbon dioxide (CO2) from working muscle and the recycling of lactate to glucose. In the adrenal gland, vitamin C is necessary for the production of epinephrine, which acts to release free fatty acids (FFA) from adipose tissue.
Consuming optimal amounts of micronutrients is therefore vital to high levels of athletic performance by ensuring optimal fuel utilisation and delivery and removal of key gases to and from working muscles.
Culp (2015) suggests that athletes have higher micronutrient consumption needs than the general population. This is because athletes have higher rates of energy metabolism and need their bodies to function at intense levels. In addition, exercise stresses the metabolic pathways where vitamins and minerals are utilised and may also result in biochemical adaptations that increase micronutrient needs. Finally, routine exercise may also speed up the turnover and loss of vitamins and minerals from the body.
The National Strength and Conditioning Association (NSCA) provides the following effects of insufficient intake of micronutrients for athletic performance.

As you can see, the effects of micronutrient imbalance through either low intake, increased losses, or a combination of both have wide-ranging effects on almost every facet of athletic performance from endurance to strength and even recovery from exercise.
But do athletes need to use supplements to meet the increased need for micronutrients, or will increasing total calorie consumption to meet increased energy demand take care of this? Here are some recent findings from studies examining this:
| Micronutrient supplementation is common in athletes. A meta-analysis by Knapik et al (2016) suggested over 50% of athletes were taking vitamin and mineral supplements and that elite athletes were taking more supplements than non-elite athletes. |
| Most evidence indicates that athletes competing in sports with high energy requirements are likely to have increased micronutrient requirements, however there is currently insufficient data to quantify how much more they need (Volpe, 2007). |
| Increased iron intake may be required in endurance athletes who maintain high levels of volume in training, particularly when full recovery isn’t allowed. Mackay et al (2019) found that iron stores were depleted in endurance athletes over a 6-week training period by between 25-40% (particularly in female athletes). The authors also found that these deficiencies could be easily avoided by increasing the consumption of iron-rich foods (or supplementation if on a restricted diet). |
| If athletes with high energy requirements are meeting those needs with a well-balanced diet, then their levels of micronutrient intake will also increase naturally. However, there may be certain situations where further focus is given to particular micronutrients. Examples of such situations include extra requirements for sodium and zinc for athletes with high sweat rates, menstruating female athletes and iron needs, or iron and B12 requirements for athletes with specific dietary preferences (vegetarians or vegans) to name a few (Volpe, 2007). |
| Some micronutrients might also be more of a concern for particular sports. For example, vitamin D may become an issue for athletes who compete in winter sports, or indoor environments and iron stores may be more compromised in athletes involved in high-intensity and endurance-based exercise (Beck et al, 2021). |
| The micronutrient intake and status of athletes have been assessed in numerous studies; however, limitations exist in many of these studies, owing to the cross-sectional nature of the study design. From the published data, however, it seems that athletes who consume adequate energy and micronutrients would not benefit from supplementation (Volpe, 2007). |
As a result of unclear and at times conflicting findings from previous research, a recent literature review by Beck et al (2021) set out to answer the question of whether athletes require additional micronutrients. Their review focused on iron, vitamins C, D, E and calcium and after reviewing the available literature concluded the following:
Deficiency and supplementation
- Micronutrient supplementation in athletes without deficiencies does not improve performance.
- Excessive doses of micronutrients can have negative side effects, such as:
- Blunting the body's natural defence system (e.g., excessive Vitamin C and E).
- Impact on the absorption of other nutrients (e.g., Zinc reducing calcium absorption).
- Possible toxicity effects like nausea and headaches.
Concerns for elite athletes
- Elite athletes should be cautious due to the lack of batch testing and regulation of many supplements, which may contain banned substances.
Performance improvement with deficiency
- When deficiencies are present, supplementation can enhance performance, particularly in cases of iron and vitamin D deficiency.
- Improvements observed in deficient athletes include:
- Enhanced oxygen delivery (aerobic capacity).
- Increased muscle and bone strength.
- Reduced injury occurrence.
- Improved immune function.
- Overall enhanced training and performance.
Antioxidant supplementation
- Studies on antioxidant supplementation (e.g., vitamins C and E) to counter oxidative stress from exercise yield inconclusive results.
- While some athletes consuming antioxidants show reduced oxidative stress, it doesn't necessarily translate to improved exercise performance.
- Antioxidant supplementation might be considered in specific situations, such as:
- High oxidative stress exposure (e.g., altitude training).
- Failing to meet dietary antioxidant requirements (e.g., restrictive eating).
- High doses of antioxidants may have negative health and performance impacts.
- Current evidence does not strongly recommend antioxidant supplements for athletes; obtaining antioxidants from a balanced diet with fruits and vegetables is advised.
Vitamin D supplementation
- Vitamin D supplementation may benefit athletes with darker skin or those training in low sunlight conditions (e.g., winter or indoor athletes).
- Athletes should have their vitamin D levels tested for deficiency before considering supplementation.
Overall recommendations
- To ensure adequate intake of all micronutrients, athletes should consume a variety of foods from all food groups and maintain an energy intake that meets their training requirements.
Key takeaways from research findings
- Athletes can meet their micronutrient needs through a well-balanced diet aligned with their energy requirements.
- There is no performance advantage for athletes when consuming excess micronutrients alongside a well-balanced diet.
- Athletes with diagnosed deficiencies may benefit from micronutrient supplementation.
- Athletes adhering to restrictive diets, such as vegans or vegetarians, and those in chronic energy deficits, may also benefit from supplementation.
- Increased micronutrient intake may support athletes in specific exercise scenarios, such as iron and vitamin E for high-altitude training and vitamin D for extended indoor or low-light training.
- Elite athletes should ensure supplement safety and avoid banned substances.
- Excessive doses of micronutrient supplements can lead to adverse side effects.
As a personal trainer, it's important to offer your clients a straightforward guideline. Ensure their daily nutritional needs are met by incorporating a variety of foods from essential food groups. This dietary approach is likely to fulfil their micronutrient requirements effectively.
In cases where a client suspects a deficiency in a specific micronutrient, it's advisable to refer them to a qualified healthcare professional. They can accurately diagnose any deficiencies and provide appropriate recommendations before considering any supplementation.
Supplements used to enhance exercise performance are obviously of keen interest to competitive athletes. These can range from banned substances like steroids which can have potent effects on muscular development, to dietary supplements that are proposed to increase performance from consumption pre, during and post exercise.
For the purposes of this topic, we will discuss what the research has found in relation to three of the most commonly used supplements used by both recreational and elite athletes looking to provide an additive effect to their training including:
- Protein powders
- Pre-workout supplements
- Creatine monohydrate.
Let’s look at the evidence-based effectiveness of these products in assisting the elements of performance they are typically taken for and how they are best used.
Protein powders

Protein powders come from a variety of different sources. The most common of these are:
- Whey – derived from cow’s milk. This is probably the most common form of protein powder consumed. Whey is often regarded as one of the highest-quality protein powders due to its favourable amino acid profile (particularly concerning the BCAA’s Leucine, Isoleucine, and Valine) and easy absorption. Whey can be either:
- Concentrate - considered a lower-quality protein product due to limited refinement meaning levels of carbohydrate and fat remain higher
- Isolate - a more refined product that contains a minimum of 90% protein by weight. This is the most common form consumed by athletes. Or;
- Hydrolysate - which has been treated with either heat, enzymes or acids to “pre-digest” the product by breaking some of the peptide bonds (for rapid digestion).
- Casein – also derived from cow’s milk (the curds). This form of protein in slower to digest as it “curdles” in the stomach’s acidic environment. It is widely used by body builders at night for a steady release of protein overnight.
- Whey/Casein blends – there has been some evidence that combining these two common forms of protein powder leads to a more complete (and prolonged) amino acid balance in the body when compared with whey intake alone. Some studies have shown an increase in muscle hypertrophy (but not strength) from use of a blend (Jager et al, 2017). Blends of whey and soy protein did not achieve the same outcomes.
- Egg protein – is more obscure than milk-based protein supplements (and often more expensive). Useful for those who have a dairy allergy.
- Plant-based proteins – considered by many to be “lower-quality” proteins as many are “incomplete” in terms of essential amino acid profile. However, plant proteins can achieve “complete” status if two or more plant proteins are combined and they are fortified with BCAAs (Some plant proteins can be more difficult to digest and absorb than animal-derived products. Common sources of plant protein powders are pea, rice and soy.
Let’s start by looking at what the research says about the effectiveness of plant-based protein powders as compared to animal sources. The following information comes from Jager et al (2017) which details the official position stand of the International Society of Sports Nutrition:
- Soy is the most researched plant protein. Research has consistently shown that it is a lower-quality protein source than milk derivatives. While soy is considered a complete protein, it contains lower amounts of BCAAs than milk. It may also have the potential to inhibit growth factors and muscle protein synthesis.
- Many plant-based proteins require larger intakes to elicit the same effect. When soy and grain-based proteins were compared with dairy proteins, it took a doubling of the intake of the plant-based proteins to achieve the same muscle protein synthesis.
- With proper supplementation and careful nutritional choices, it is possible to have complete proteins in a vegetarian diet. However, by consuming high-quality, animal-based products (meat, milk, eggs, and cheese) an individual will achieve optimal growth with greater ease than those ingesting only plant proteins.
A recent meta-analysis by Lim et at (2021) weighed in on the same topic. They screened 3081 studies on the topic and deemed only 18 were worthy of inclusion in the analysis. Overall conclusions suggested that the protein source did not affect changes in absolute lean mass or muscle strength, however, there was a favouring effect of animal proteins on the percentage of lean mass. Younger adults (under 50) were also found to gain both absolute and lean mass better on animal protein. The authors concluded that collectively, animal protein tends to be more beneficial for lean mass accrual than plant protein, especially in young adults.
The effectiveness of protein powders
The main reason athletic populations consume protein powders is to enhance muscle protein synthesis for recovery from exercise and the growth of muscle tissue (for improved performance gains). So, how effective are protein powders at achieving this?
A systematic review and meta-analysis by Morton et al (2018) set out to answer this question. This is the largest meta-analysis on this subject to date. The authors included the data from 49 studies including 1863 trained and untrained participants (men and women of different ages). The studies encompassed a wide range (and duration) of resistance training approaches and included various protein sources including whey, casein, soy, pea, and protein blends and compared these with real food intakes). The authors made the following conclusions suggesting that protein powder supplementation when used alongside regular resistance training:
- Significantly enhanced strength as measured by 1RM lifts but had no significant effect on maximum voluntary contraction of muscle. The authors concluded that while taking protein supplementation offered some small additional benefit to conducting resistance training on a balanced diet, resistance training was a far more potent stimulus for increasing muscle strength than the form in which protein was ingested.
- Had no significant effect on total body mass but did significantly increase fat, free mass (lean tissue) and increase the cross-sectional area of muscle fibres.
- Was more effective for more experienced resistance-trained athletes than novices and the effects reduced as people aged.
The authors also noted the supplementation with protein powder did not achieve any further enhancement at levels over 1.6g/kg/day. When the protein supplement was taken did also not seem to have an effect on protein synthesis. For example, studies that took the protein powder straight after training had no additional effect on those who took some time later.
Morton et al (2018) did however indicate that well-trained resistance athletes may benefit more from protein powder supplementation directly after training, as they have a smaller potential for muscle growth and a higher protein turnover post-exercise than untrained populations. A systematic review by Pasiakos et al (2014) agreed with this finding. These authors concluded that for untrained individuals, consuming supplemental protein likely has no impact on lean mass and muscle strength during the initial weeks of resistance training. However, as the duration, frequency, and volume of resistance training increase, protein supplementation may begin to promote muscle hypertrophy and enhance gains in muscle strength in both untrained and trained individuals.
Thomas et al (2016) explain the likely reason behind the reduced effect of protein supplementation as we age. They suggest that older populations develop an anabolic resistance as the expression and activation proteins responsible for muscle growth are reduced with age. This causes a blunted anabolic response compared with younger athletes. It appears that protein supplementation will only aid older athletes engaged in resistance training if they do not already meet minimum protein requirements in their daily diets.
The significance of protein powder quality
Morgan et al (2021) performed their own meta-analysis on protein source and quality and its effect on muscle growth. In this review, 27 appropriate studies were separated into those that used high-quality protein powders (containing over 2g of Leucine, other essential BCAAs and having high digestibility) and low-quality protein powders (containing less than 2g of Leucine, less other essential BCAAs and having lower digestibility). High-quality proteins were mostly whey isolates and hydrolysates, while lower-quality proteins included mostly plant-based proteins and some casein proteins. The review also split the studies into those who ingested protein powder without any exercise, those who ingested protein powder after one bout of resistance exercise, and those who ingested protein powders ongoingly after longer-term resistance training programmes. Here are the key findings:
- Protein quality was highly associated with muscle protein synthesis (MPS) rates in the following groups:
- High-quality protein had a significant effect on older but not younger adults in the non-exercise group compared to low-quality protein.
- High-quality protein had a significantly better effect on MPS and strength in all age groups that took it following a single bout of resistance training.
- High-quality protein had a more significant effect on MPS and strength gains in those on longer resistance training approaches
- Lean body mass did not appear to be affected by the quality of protein ingested by the longer-term resistance training group.
In summary, after reviewing the research, higher-quality proteins seem to offer greater benefits for older individuals who don't engage in resistance exercise. They lead to more significant gains in strength after both single and prolonged bouts of resistance training. However, it's important to note that they may not necessarily promote greater increases in lean body mass when compared to lower-quality proteins.
Pre-workout supplements

As the name suggests, a pre-workout supplement is designed to be consumed prior to exercise with the aim of enhancing training performance. Pre-workout supplements are most commonly consumed as a powder mixed into water, but capsules, chews and pre-mixed drinks are also becoming common. The composition of these products varies considerably, which makes comparisons of their effectiveness difficult.
Jagim et al (2019) set out to identify the common ingredient profiles of the top 100 selling pre-workout supplements on the market and concluded that the most popular ingredients in these supplements and the manufacturer's reasons for including them were:
- Beta-alanine (87%) - A non-essential amino acid that aids in the production of carnosine. Carnosine is thought to play a role in muscle endurance during high-intensity exercise by regulating acidity.
- Caffeine (86%) - Thought to exercise performance by stimulating activation hormone production, mental focus and fat metabolism.
- Citrulline (71%) - A non-essential amino acid thought to reduce ratings of perceived exertion, decrease muscle soreness and increase power output through mechanisms leading to increased blood flow.
- Tyrosine (63%) - A non-essential amino acid that the body can create from another amino acid called phenylalanine. It is thought to increase energy and endurance and improve focus and alertness.
- Taurine (51%) - While many suggest taurine is “essential” it is another non-essential amino acid. It is thought to enhance muscle contraction, delay muscle fatigue and promote fat metabolism.
- Creatine (49%) - Is an amino acid derivative thought to increase strength, power and high-intensity exercise performance.
- Niacin (48%) - Also known as vitamin B3. Thought to assist the efficient metabolism of energy for exercise.
Jagim et al (2019) suggested that the average amounts of many of these ingredients (per suggested serve) did not align with the evidence-based dosing recommendations for enhanced performance. For example, the average amount of creatine included less than the minimum 3g/day suggested for performance enhancement with only 29% of the products tested having the minimum ergogenic amount. Similarly, the average listed amount of beta-alanine was well below the minimum suggested performance enhancement dose wih only one product of those tested containing a dose higher than the recommended ergogenic dose of 4g/day. Similar findings were reported for other ingredients including citrulline and arginine.
While the average amount of caffeine in the tested products was 254mg which sits above the 210mg required to meet the lower threshold for a recommended dose, this would only meet the threshold for those 70kg or under (which is likely to be a small portion of resistance-trained athletes). Studies have indicated that caffeine intakes of closer to 6mg/kg of body weight are likely needed to create an ergogenic benefit for well-trained resistance athletes which suggests the average caffeine content of the tested products may also be insufficient for those looking to make additional strength or power gains (Jagim et al, 2019).
One ingredient that was included in most products at an elevated level was Niacin. The average amount of Niacin per suggested serve (26g) was getting close to the tolerable upper level of 35mg/day. Several studies have linked high intakes of Niacin with acute hepatitis and liver failure in healthy adults. This means there is a potential risk associated with the use of pre-workout supplements particularly if having them more than once a day (Jagim et al,2019). This would also carry a risk for excessive caffeine consumption, particularly if athletes are consuming other caffeine sources throughout the day. Noted issues coming from excessive caffeine ingestion include tachycardia (irregular heart rate), heart palpitations, headaches, anxiety and sleep disturbance (Sepkowitz, 2013).
The effectiveness of pre-workout supplements
A literature review by Harty et al (2018) set out to answer that question. Here are the key findings of their report:
- Acute ingestion of a multi-ingredient pre-workout supplement appears to have little effect on maximal force production (i.e. strength), however, those that contain caffeine may help to delay the effect of fatigue on repeated repetition lifting. This means while absolute strength was not improved, the ability to perform full repetitions in subsequent sets was improved.
- Some studies investigating the effect of a pre-workout supplement reported an increase in repetitions to fatigue, whereas others found no clear improvement. Other studies found improvements in some body parts but not others (e.g. improved leg press repetitions, but not bench press). Despite the mixed results, on balance, there appears to be a trend towards pre-workout consumption assisting muscular endurance performance as measured by repetitions to failure.
- Pre-workout supplementation may also improve total exercise volume completed with the results of studies covering weighted exercise, bodyweight exercise and repeated sprinting.
- Results from studies examining the effect of pre-workout supplements on power production are conflicting. Most research has indicated that no improvement was shown in one-off power efforts, but that there appears to be a tendency towards the ability to retain upper-body power and anaerobic sprints in repeated effort approaches.
- Very little evidence exists for the use of a pre-workout supplement for endurance exercise with only one study showing that a pre-workout supplement may enhance time to exhaustion during treadmill running. The few remaining studies that have been completed reported no effect of pre-workout ingestion on endurance performance (in both cycling and running).
- The results of several studies suggest that the use of a pre-workout supplement may improve reaction time as well as accuracy during hand-eye coordination tasks.
- A limited number of studies have looked at the effect of pre-workout supplement intake on fuel use during exercise with limited evidence to suggest any effect on fat utilisation as a fuel.
The results of this review would suggest that any improvements resulting from pre-workout ingestion are preliminary at best and that more significant research is needed in this area. The high consumption rates of these products by athletic populations (particularly in resistance training circles) indicate that those who use them must feel some form of benefit in their use (even if the evidence is not there to back this up). In their review Harty et al (2018) also explored the subjective feelings of those who use these supplements and despite conflicting findings concluded that acute use of pre-workout supplements does appear to improve self-reported subjective measures of focus, fatigue, alertness and energy levels.
The safety of pre-workout supplements
The final part of the review by Harty et al (2018) looked at the safety implications of regular pre-workout use. These were their conclusions:
- To date, relevant literature suggests that the consumption of most pre-workout supplements appears to be relatively safe, with minimal reports of adverse effects during studies. However, it should be noted that the vast majority of studies were less than 8 weeks in duration, which means the long-term effects of ingestion are unknown. Another important point to raise is that adverse effects were only ever reported as a group mean with no “individual severity” of adverse effects reported in the literature.
- Research that has been conducted specifically to analyse the effects of these supplements on health has reported the following effects after acute or short-term (10-day) chronic ingestion:
- No changes to liver function
- Minor reductions in kidney function
- No effect on blood or cardiovascular function during exercise but reports of higher post-exercise heart rate and diastolic blood pressure. Most of these effects are in line with caffeine ingestion effects.
- The authors concluded that it is unlikely that any longer-term studies on pre-workout supplements will be funded until manufacturers are required to show the effects of long-term consumption by National health organisations. More on this soon.
- One final area of concern is the contamination of these products. Many of the products tested in the literature have contained heavy metals, potent stimulants and various banned substances which may have an effect on human health if consumed long-term.
Comparing the effectiveness of pre-workout and caffeine alone

Pre-workout supplementation can be expensive. Caffeine is one of the main ingredients in most pre-workout supplements. The average number of ingredients in pre-workout is around 15 (Jagim et al,2019), but does adding all the other ingredients make a noticeable difference?
Most of the literature actually points to caffeine causing either the same effect or in some cases even more performance effect than pre-workout supplements. A 2022 study by Kruszewski et al compared pre-workout consumption to caffeine consumption alone and found that bench press repetition volume was greater after caffeine consumption alone than the pre-workout and that subjects reported no difference in psychological measures. Lane et al (2019) also reported no differences in power maintenance of upper and lower body tasks between pre-workout and caffeine consumption alone. It would therefore appear that consuming caffeine alone will elicit (at least) comparable effects to more expensive pre-workout “blends”.
There must be some reason they include all the other ingredients, right? Yes. Each of the other ingredients has been shown to improve specific performance outcomes in their own trials, however, the amounts used in these studies that lead to improved performance outcomes far exceeded the amounts commonly found in pre-workout supplements. This means while the advertising these supplement producers use to promote the effects of their products is essentially evidence-based, it is very unlikely you will be receiving a performance-enhancing dose of each of these substances in these products.
Tolerance development with pre-workout supplements
While there is little evidence-based research to confirm this, Cooper and Joshi (2023) suggest that you can build up a tolerance to the effects of pre-workout supplements and suggest that athletes should “cycle off” using pre-workout for 6-8 weeks to elicit the best results from using it. This anecdotal evidence is likely to stem from research into the tolerance observed in chronic caffeine consumption. Van de Walle (2020) reports that caffeine tolerance does exist. This author references a study by Lara et al (2019) which compared the daily effect of caffeine consumption on cycling power. When compared with a placebo group, the caffeine group exhibited a 4-5% improvement in cycling power for the first 15 days, but this improvement decreased after this point and the cyclists returned to performances in line with the placebo group. Similar findings have been reported in other studies. Most of the literature supports the cycling of caffeine ingestion rather than the alternative approach of simply continuing to increase caffeine intake over time to elicit the same results.
There may be a slight benefit towards the use of pre-workout supplements for increased performance and it appears that if they are used as recommended, there is little evidence that they are harmful. While there is little evidence to support their use, they may offer more subjective benefits like reduced feelings of fatigue and alertness which could prompt more effective training sessions. What is clear is that there needs to be more research done in this area, particularly on the longer-term effects of using these products.
Creatine

Creatine is a dietary supplement that is thought to increase muscle performance. It is most often used by those involved in resistance training who seek an increase in strength (and size), however, its effect on endurance performance and muscle recovery has also been extensively studied. Lanhers et al (2015) suggest that creatine is the most widely used supplementation to increase strength performance.
Types of Creatine
There are a number of creatine supplements available on the market. Here are the most popular:
- Creatine monohydrate: Creatine bound to water molecules. By far the most commonly bought and consumed form of creatine supplement. It is also the most widely researched form of creatine and has been suggested to have a more physiological impact on intramuscular levels of creatine than other forms.
- Creatine ethyl ester: Creatine bound to ester salts. This was originally thought to increase the bioavailability of creatine. Subsequent comparison studies with creatine monohydrate did not show any additional benefit.
- Creatine hydrochloride (HLC): Creatine binds to part of hydrochloride molecules which lowers the pH (raises acidity). Only benefit appears to be a reduction in stomach cramps compared with other forms.
- Buffered creatine: A more alkaline product where creatine is buffered with sodium carbonate and bicarbonate. No clear evidence of any additional benefit over other forms.
- Creatine magnesium chelate: More claims of greater bioavailability, but lacking evidence-based support.
On the basis of research that has been completed, creatine monohydrate should be the preferred source of supplementation as it is generally well tolerated and has a wealth of evidence associated with its effectiveness. For this reason, the remainder of this topic will focus on creatine monohydrate.
Mechanism of action for creatine supplementation
Creatine monohydrate supplementation is thought to increase the phosphocreatine/creatine ratio in skeletal muscle tissue, thereby increasing the capacity for more rapid production of adenosine triphosphate (ATP) during repeated high-intensity exercise tasks (Wu et al, 2022). Put simply, creatine supplementation increases your muscle store of phosphocreatine, which can be used to make new ATP during intense exercise. This allows more efficient production of ATP to allow for continued energy production to support high-intensity, short-duration efforts like heavy lifts.
Effects of Cceatine supplementation on hypertrophy
Muscle growth appears to be enhanced by creatine supplementation particularly in young healthy populations (Wu et al, 2022), however, training stimulus needs to be adequate for any effect. Reported increases in lean mass following creatine supplementation have at least partly been attributed to water retention in muscle tissue. This comes about from the greater osmotic pressure from increased creatine in muscle resulting in muscle cell swelling. This effect is often somewhat reversed when supplementation is stopped, but a net gain in muscle growth is still commonly found after supplementation cessation (Wu et al, 2022).
Effects of creatine supplementation on strength
Lanhers et al (2015 and 2017) conducted two meta-analyses covering 113 research articles. One explored the effect of creatine monohydrate supplementation on upper body strength and the other on lower body strength. The main findings of the analyses were:
- Supplementation with creatine monohydrate improved upper body strength performance (mainly in the pectoral muscles) and lower limb strength performance (mainly in the quadriceps).
- Across the studies, creatine supplementation led to bench press performance increases of approximately 5.3%, barbell squat performance by 8% and leg press by 3%.
- There were no reported differences in regard to age, gender, or training level for upper body performance outcomes, however, untrained subjects exhibited a better response to creatine supplementation with lower body exercise (31% increase in performance vs. 14% in well-trained subjects).
- Creatine supplementation regimes that included “loading” and “maintenance” phases did not elicit greater results than short-term loading approaches.
- Equal benefit was seen when subjects performed isolated strength lifts vs. compound lifts and when unilateral exercises were performed compared to bi-lateral exercises.
Effects of creatine supplementation on endurance
While the effects of creatine monohydrate supplementation on strength are well documented, far less research has been conducted in the area of endurance performance. Fernande-Landa et al (2023) conducted a meta-analysis on the effects of creatine monohydrate in endurance performance in trained athletes. Their review included 13 quality studies. The results of this review concluded that the use of a creatine monohydrate supplement was ineffective in improving the endurance performance of trained athletes beyond durations of 3 minutes. This would suggest that the use of creatine supplementation is unwarranted by endurance athletes.
Effects of creatine supplementation on muscle recovery
There has been some suggestion that supplementation with creatine monohydrate might reduce muscle damage in athletes leading to enhanced recovery. Doma et al (2022) set out to explore these claims with their meta-analysis and review of 23 research articles. The authors concluded that supplementation with creatine did result in lower indirect muscle damage markers at 48-90 hours post a single bout of exercise, but that muscle damage markers were significantly higher at the 24-hour post exercise mark when a chronic training approach was taken (i.e. daily exercise). The authors also reported that those consuming creatine in experiments showed lower inflammation and oxidative stress markers for up to 90 hours post a single exercise bout and lower DOMS (delayed onset of muscle fatigue) at 24-hours post a single exercise bout. Interestingly these effects seemed to be reversed when subjects were subjected to a chronic training approach (I.e. when they were not allowed full recovery before training again).
These findings led the authors of this review to conclude that creatine ingestion led to more favourable recovery outcomes from a single bout of exercise but seemed to produce the opposite effect following repeated exercise bouts over days. This raised the question of whether creatine supplementation during chronic training approaches might lead to increased levels of exercise induced damage. To date, this effect has not yet been explored.
The following video summarises the key benefits and potential negative effects of creatine supplementation. It also discusses the best approach for using creatine supplementation.
Common questions and misconceptions about creatine supplementation
An internationally renowned group of experts got together to answer common questions and clear up misconceptions about creatine supplementation by reviewing the scientific literature that exists to date. Antonio et al (2021) created the following list of evaluative findings as supported by evidence-based research:
Safety and general use
- Creatine supplementation does not always lead to water retention.
- Creatine is not an anabolic steroid.
- Creatine supplementation, when ingested at recommended dosages, does not result in kidney damage and/or renal dysfunction in healthy individuals.
- The majority of available evidence does not support a link between creatine supplementation and hair loss/baldness.
- Creatine supplementation does not cause dehydration or muscle cramping.
- Smaller, daily dosages of creatine supplementation (3-5 g or 0.1 g/kg of body mass) are effective. Therefore, a creatine ‘loading’ phase is not necessarily required. Results appear similar regardless of the approach.
- Other forms of creatine are not superior to creatine monohydrate.
Benefits for various groups
- Creatine supplementation appears to be generally safe and potentially beneficial for children and adolescents.
- Creatine supplementation and resistance training produce the vast majority of musculoskeletal and performance benefits in older adults. Creatine supplementation alone can provide some muscle and performance benefits for older adults (even without exercise).
- Creatine supplementation can be beneficial for a variety of athletic and sporting activities (not just strength and power sports). Any sport that involves short sharp bursts of energy can benefit from creatine supplementation.
- Creatine does not only offer effects for females. Creatine supplementation provides a variety of benefits for females across their lifespan.
Body composition and performance
- Creatine supplementation does not increase fat mass (in fact, most studies reveal reductions in fat mass).
Choosing nutritional supplements
As we have previously discussed, the regulation of dietary supplements in NZ is quite limited. This means there is a lot of trust placed in the manufacturers of dietary supplements to ensure that the product they put to market is safe to consume and contains what it says it does on the label. There is increasing evidence that this is not always the case. There are many examples of athletes who have been exposed to banned substances through the consumption of seemingly innocuous health supplements.
This situation is far more prevalent than you might think. In fact, most international sports bodies now advise athletes to abstain from using any nutritional supplements (de Hon and Coumans, 2007). This is of course not something that athletes abide by, with suggestions that 93% of NZ athletes use supplements (Curtis et al, 2015).
This situation is far more prevalent than you might think. In fact, most international sports bodies now advise athletes to abstain from using any nutritional supplements (de Hon and Coumans, 2007). This is of course not something that athletes abide by, with suggestions that 93% of NZ athletes use supplements (Curtis et al, 2015).
Elite athletes are subjected to routine anti-doping tests for prohibited substances and methods, often with no prior notice, both within and outside of competitions. Many athletes who have returned positive tests for banned substances have claimed that their use of these substances was inadvertent. While it would be easy to assume the worst (that they were all cheating) there is significant evidence that common supplements from vitamins and minerals, protein powders, joint support supplements and common over-the-counter medications for colds etc. either contain banned substances or have been contaminated with banned substances (Mottram, 2015).
In 2016, LGC (an established international life sciences measurement and testing company) conducted a supplement survey that included the testing of over 50,000 samples from 67 nutritional supplements. The range of supplements tested included:
- Amino acid and protein supplements
- Creatine
- Weight management supplements
- Hormone Boosters
- Pre- and Intra-workout supplements
- Minerals
- Multivitamins
- Post workout rehydration supplements including sports drinks
The forms that these supplements came in included bars, capsules, gels, liquids, powders and tablets. Here are the key findings of the testing:
- One in five (19%) of the 67 products tested contained one or more substances that would be considered prohibited within sport.
- The most common contaminant found was a stimulant called AMP Citrate which was found in 7 products. 25% of the banned substances found were in the form of anabolic steroids, while the other 75% were stimulants (one of these was methamphetamine).
- Weight management supplements yielded the most banned substances (31%) with Pre-workout supplements the second most common (23%).
- Of all of the substances tested, powders returned the highest numbers of banned substances making up 69% of all findings, with capsules and tablets next.
- A number of supplements did not indicate the banned substance at all on the label, or included amounts on the label that were lower than what was detected in the product.
- The authors of the survey concluded that athletes remain at risk of a potential career-ending doping violation by taking products that are not subject to rigorous banned substance screening. It is therefore vital that athletes who are subject to routine doping control ensure they select only those products which have been subject to appropriate quality control/testing programs.
High-Performance NZ agrees. They produced a short article warning of the importance of athletes choosing their dietary supplements carefully. The main points from the article include:
- No supplements are approved by the World Anti-Doping Association (WADA) or Drug-Free Sport NZ.
- NZ athletes access dietary supplements from all over the world. Regulations in these countries may be different to NZ.
- While NZ-made supplements are regulated under the Dietary Supplements Regulations Act (1985) they may still contain banned substances as there is no pre-approval process currently in NZ.
- If an athlete chooses to consume a supplement, they should only choose those that have been independently batch tested as this substantially reduces the risk of consuming a product contaminated with banned substances. Any product used should have a batch certificate that exactly matches the product. Accredited and independent batch-testing services are available worldwide and their logos can often be found on batch-tested products. The most trusted are:
- Once a product has been batch tested, a certificate of analysis (COA) is awarded, and the batch number is usually made publicly available on the websites below (and on the manufacturer's website) to prove it has been tested and passed.
- Athletes should keep in mind that contamination can occur in one batch of a product and not others, so they should never continue to use the same product over long periods and assume it has passed testing.
- Recent supplement contamination alerts can be found here on the MedSafe website: MedSafe: Safety Communications
How to find a batch number on a supplement
The product batch (or Lot) number is often located next to the expiry date on the bottom of a container or on the lid. It is usually a number preceded by a “B”, for example:

Upskilling
Any trainer working with elite athletes, should be fully aware of anti-doping legislation and be able to keep their clients safe and informed. Drug-Free Sport NZ has developed a series of educational courses for both athletes and support staff to take for free online to ensure they are fully informed of best practice when it comes to avoiding the inadvertent (and purposeful) consumption of banned substances. You can access these courses here:
The information above has given detailed coverage of the most commonly studied dietary supplements taken to support health and performance. In recent years, a number of additional foods have been much discussed in terms of potential health and performance benefits. These foods have been referred to by many as “functional” or “super” foods and are thought to contain specific bioactive compounds. In simpler terms, they contain micro-nutrients thought to influence cellular activities, offer additional benefits besides calories and have a potentially positive effect on performance. Many of these foods have been traditionally consumed as “health” foods based on anecdotal evidence, but now have scientific evidence to support their use. In the last decade, the “functional” nutrients found in these foods have been studied in “supplement” form to assess their effect on performance.
Let’s find out what the research has to say about the following “functional” nutrients:
- L-citrulline (from watermelon and other melons).
- Tart cherry (Montgomery cherry).
- Blueberries and blackcurrants
- Beetroot (nitrates).
- Bromelain (from pineapple).
- Curcumin (from tumeric).
- Collagen (from gelatine).
- Athletic Greens - AG1.
- Probiotics.
L-citrulline

L-citrulline is an amino acid that can be metabolised into arginine. Arginine is used in the synthesis of nitric oxide which plays a role in cardiovascular and immune health. Nitric Oxide acts is thought to act as a vasodilator improving blood flow. Watermelon is a great source of L-citrulline and also contains lycopene and Vitamin C which are anti-inflammatory antioxidants.
A number of studies have looked at the potential performance effect of L-citrulline. It has been suggested that the benefits of L-citrulline supplementation may include improved muscular endurance, resistance to fatigue during exercise and enhanced recovery after exercise making it most beneficial to endurance-based athletes. Gonzalez and Trexler (2020) performed a review of the current literature on the potential for L-citrulline to enhance performance and reported the following:
- Oral ingestion of L-citrulline results in increased plasma citrulline, arginine and nitric oxide, but does not necessarily result in improved blood flow (evidence is scarce). However, several studies have shown that L-citrulline supplementation can enhance exercise performance and recovery.
- The most common form of supplement containing L-Citrulline is Citrulline Malate which provides a 1:1 or 1:2 ratio of citrulline to malate. Studies that have reported a performance-enhancing effect of citrulline malate have tended to use a 6-8g/day dose which would yield around 3g of L-citrulline
- L-citrulline ingested 60-90 minutes prior to exercise seems to most reliably enhance performance, however, research has not consistently shown that a single dose of L-citrulline improves endurance performance. Based on current evidence, dosing with L-citrulline over 7 days seems the best approach. The minimum effective dose seems to be around 3g/day, while the maximum effective dose may be closer to 10-15g/day.
- L-citrulline supplementation may also aid the recovery process by diminishing perceptions of muscle soreness and reducing plasma lactate levels.
- The effect of L-citrulline supplementation on high-intensity exercise and strength is less clear with studies in this area returning conflicting results. A recent meta-analysis by Trexler et al (2019) found that L-citrulline supplementation might yield a small improvement in these modes of exercise but that further research was necessary.
It appears the effects of L-citrulline can be obtained through either supplementation or by drinking watermelon juice (with recovery effects, in particular, being enhanced more with juice). However, the practicality of consuming watermelon juice may favour supplementation. There is between 0.7 and 3.6mg of L-citrulline in 1 gram of watermelon. A small watermelon weighs around 3kg. That means a whole watermelon yields around 11g of L citrulline. with a cup of watermelon juice yielding 2-2.5g. This means around 3 cups of watermelon juice would have to be consumed daily prior to exercise to get the effects noted in the research.
L-citrulline can be bought from most supplement stores (or online).
Tart cherry (Montmorency cherry)

These cherries are high in "Polyphenols" which provide antioxidant & anti-inflammatory properties. A quick search on what benefits these cherries can elicit suggests they can:
- Reduce symptoms of rheumatic conditions by reducing inflammatory markers.
- Accelerate recovery following strenuous, high-volume exercise.
- Reduce oxidative stress during exercise.
- Reduce muscle soreness.
- Improve recovery of muscle function.
- Reduce enzymes associated with muscle tissue damage (creatine kinase (CK), and aspartate aminotransferase (AST)).
- Improve the quality of sleep
The following image shows, tart cherries are particularly high in antioxidants compared with other plant sources:
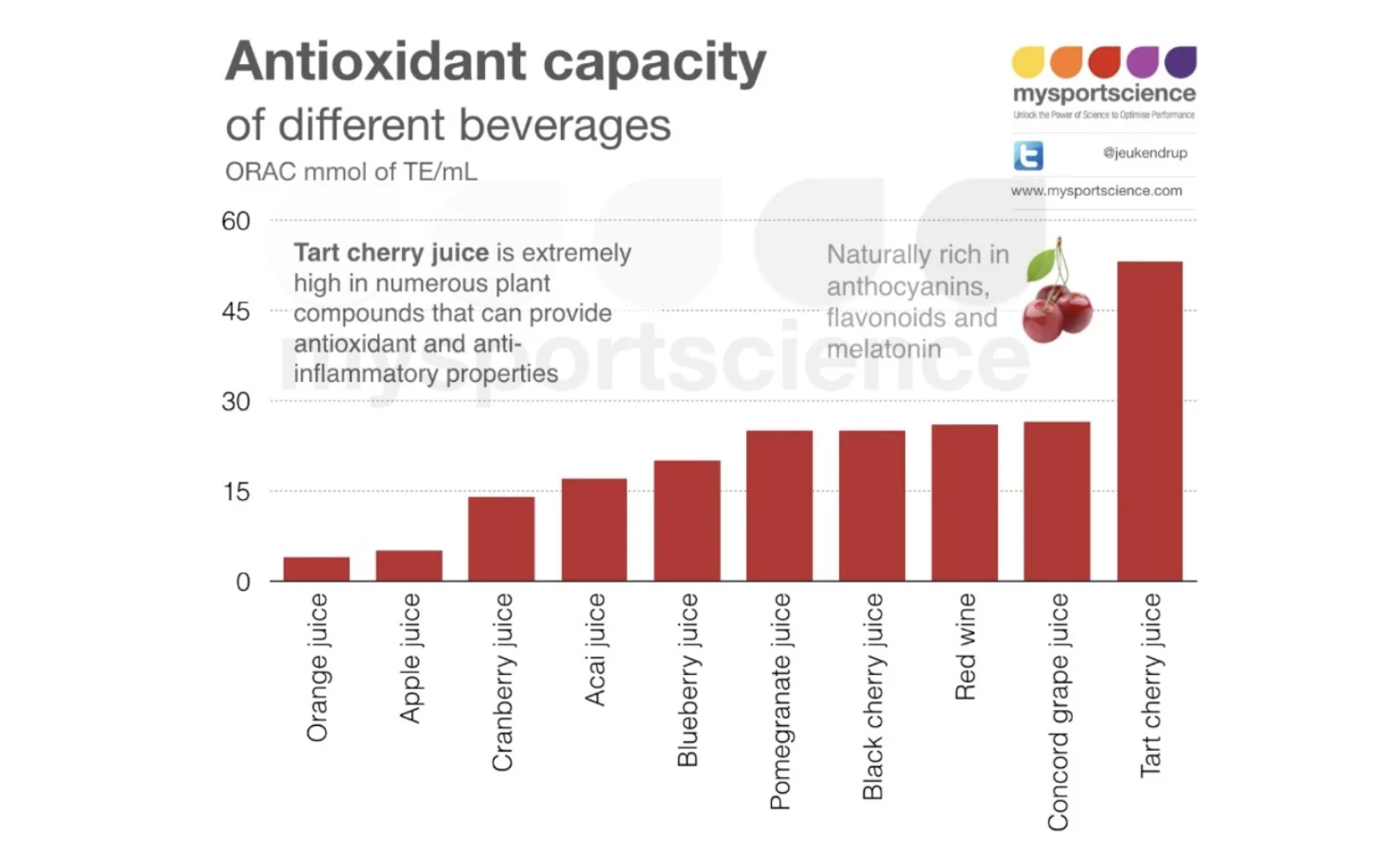
This realisation led to numerous studies being conducted. There are a number of inconsistencies in their findings as shown in the following table:
| Study | Metabolic/Damage | Function | Soreness | o2 stress | Inflammation |
|---|---|---|---|---|---|
| Connoly et al 2006 | Damage | Y | Y | - | - |
| Kuehl et al 2010 | Metabolic/Damage | - | Y | - | - |
| Howatsen et al 2010 | Metabolic/Damage | Y | N | Y | Y |
| Bowtell et al 2011 | Damage | Y | N | Y | N |
| Kastello et al 2014 | Damage | Y | Y | N | Y |
| Bell at el 2014 | Damage | - | N | Y | Y |
| Bell at el 2015 | Damage | Y | N | N | Y |
| Bell at el 2016 | Metabolic/Damage | Y | Y | N | Y |
| TOTAL | - | 6/6 (100%) | 4/8 (50%) | 3/6 (50%) | 5/6 (83%) |
A meta-analysis conducted by Hill et al (2021) included 13 studies on the effects of these cherries and concluded that tart cherry supplementation had:
- a small but significant effect in reducing muscle soreness post-exercise
- a moderately enhanced effect on recovery of muscle strength and power post-exercise
- a large effect on the recovery of performance of jump height
- a small (but significant) effect on the recovery of sprint times
- a small effect on levels of C-reactive protein but non-significant effects on creatine kinase and other muscle tissue damage enzymes.
The authors concluded that supplementation with tart cherry can aid the recovery of muscle function and reduce muscle soreness following strenuous exercise. The most commonly used dose of tart cherry concentrate was 30ml twice daily (1-7 days prior and 1-5 days after). Because this is the equivalent of 50-60 cherries, concentrated cherry juice is the best option). This can be bought at most NZ natural health stores (or online). There are also powder and capsule forms.
Blueberries and Blackcurrants

Blueberries are thought to contain antioxidative and anti-inflammatory properties that might assist recovery from strenuous exercise. These effects seem to stem from anthocyanins (the pigment that gives berries their red/blue/purple colourings) which have been shown to reduce cellular oxidative damage and inflammation.
This is an area in which NZ researchers have led the way. In a study by McLeay et al (2012) athletes consumed a smoothie containing 200g of blueberries along with a banana and a cup of apple juice. The control group drank a calorie-matched smoothie of the same ingredients minus the blueberries. These smoothies were consumed 5 and 10 hours prior to a muscle-damaging eccentric exercise session, then immediately, 12 hours and 36 hours after the session. The authors concluded that the blueberries appeared to accelerate recovery as measured by peak isometric strength. A similar trend was noted for concentric and eccentric strength. Additional results indicated reduced muscle damage/soreness, decreased markers of DNA and oxidative damage to muscle.
A second NZ study had athletes consume blackcurrant anthocyanin-rich extract (BAE) for 5 weeks. The extract was given to rowers 90 minutes before a strenuous rowing session. The authors concluded that the extract caused beneficial/protective antioxidant/anti-inflammatory cellular events that facilitated exercise recovery.
A systematic review by Cook and Willems (2018) suggested that performance improvements may also be possible from the ingestion of dietary or supplemental anthocyanins. The authors suggested these effects might be berry-specific as performance and recovery improvements have been noted from the use of blackcurrants, but not cherries. Performance improvements were likely the result of improved blood flow, and recovery benefits through antioxidative and anti-inflammatory pathways.
Additional health benefits of blueberry and blackcurrant consumption include:
- Lower blood pressure and maintenance of cardiovascular health.
- Protection of the liver, and reduction in liver fat buildup
- Improved insulin sensitivity in obese men and women.
- Improved immune function through increased Natural Killer (NK) cell count). These are cells that play a key role in immunity killing malignant cells and eliminating viruses.
Beetroot

Beetroot contains nitrates which are thought to increase the flow of blood and oxygen to the heart and thereby increase the amount of work that the heart can do by dilating (expanding) the arteries and veins in the body. While some studies have shown that dietary nitrate consumed as beet juice can reduce the oxygen cost of sub-maximal exercise, other studies have produced conflicting results. Beetroot has also been suggested to enhance the tolerance to high-intensity exercise and improve endothelial function (flexibility/dilation of blood vessels). From a health perspective, beetroot has also been found to reduce blood pressure and increase regional perfusion in the brain.
While many of the above findings were exciting and prompted a swift increase in the use of beetroot juice in high-performance circles, the research simply hasn’t been consistent. A quick search of “beetroot juice and performance” online will paint beetroot as a super-performance food but the research simply doesn’t yet back this up.
A meta-analysis on the effect of beetroot on high-intensity interval training by Wong (2021) concluded that beetroot consumption had little to offer in terms of improvements in peak or mean power output during HIIT or sprint interval training.
A meta-analysis on the effect of dietary nitrates (including beetroot) on endurance exercise performance by McMahon et al (2017) concluded that dietary nitrates were likely to elicit a positive effect on endurance capacity (time to fatigue), but not time-trial (race) performance.
A review of the effect of beetroot juice on performance was completed by Zafeiridis (2014). It appears that most studies have used beetroot juice containing 5-8mmol of nitrate. This equates to a minimum of 1L of beetroot juice or 0.5-1kg of beetroot. This is obviously a difficult amount for an athlete to consume. Zafeiridis (2014) concluded that the performance benefit of beetroot supplementation for athletes is simply not yet clear. Those studies did report a performance improvement after longer-term ingestion (approximately 6 days).
In terms of what to consume, it appears best to seek out beetroot juice that can provide a nitrate content of 0.1-0.2mmol/kg (6.4-12.8mg/kg). In real terms, a 65kg person would need to consume 500ml of beetroot juice, or half a kilo of beetroot. Larger people would need more like 1L a day. Luckily you can now also buy 60ml concentrated shots.
Clearly, more research needs to be done in this area before we can confidently suggest beetroot as a performance-enhancing food.
Bromelain

Bromelain is a group of enzymes found in the fruit and stem of pineapples. It belongs to the protease group of enzymes that are known to aid digestion by breaking down dietary proteins. Bromelain has been promoted as a supplement for reducing pain and swelling, muscle soreness, symptoms of arthritis, cancer and digestive problems. Other suggested benefits include anti-inflammation, immune system stimulation and the opening of airways. This has led to Bromelain supplements being sold widely as an alternative to arthritis medication and anti-inflammatory drugs (e.g. ibuprofen). While scientific support for its use in clearing the airways and improving digestive function is relatively strong, the research only has weak support for the use of bromelain as a recovery tool for exercise. While improvements have been found in terms of lower sensation of fatigue and post-exercise muscle soreness, the measures of these have been largely subjective and more scientific measures using blood markers of muscle damage have shown no effect. A small trend towards reduced inflammation has been shown, although the mechanisms behind these improvements are unknown (O’Connor et al, 2022).
It has also been suggested that for any positive effect to be seen of bromelain on it’s own, the ingestion of around 1000mg of bromelain a day is required (taken separately from food). This equates to around 20 cups of pineapple! Therefore, bromelain in supplement form would be necessary to elicit effects.
Better results for recovery have been shown when bromelain is included in smaller amounts (100mg) alongside other enzymes that break down protein with evidence-based reports of lower post-exercise soreness and better retention strength performance as the most common findings.
Overall, support for the use of bromelain as a recovery supplement is relatively weak as the potential mechanisms for how it might assist recovery are poorly understood (Bongiovanni et al, 2020).
Curcumin

Curcumin is a polyphenol that is primarily found in the spice Turmeric. It has received interest from both the medical and scientific world over the last 20 years, with over 200 clinical trials having been conducted and reporting health benefits such as:
- Anti-inflammation properties (especially related to joint pain).
- Anti-hyperlipidemic properties - reduction of blood lipid (fat) levels.
- Antioxidant properties –may support repair of DNA damaged by oxidative stress
- Reduction in lipid plaque levels in arteries (reducing blood pressure).
- Assisting digestive function
These evidence-based results prompted sports scientists to see whether there would be any benefit for athletes by reducing inflammation and pain following exercise. A meta-analysis examining the effect of curcumin on post-exercise recovery and muscle soreness was carried out by Fang and Nasir (2020) who concluded that there was strong evidence for the use of curcumin to reduce both blood markers and subjective measure of muscle soreness post-exercise. The authors finished by strongly recommending its use by athletic populations. These positive findings were backed up by Nanvati et al (2022) whose narrative review of evidence to date concluded that curcumin doses between 90-5000mg/day can decrease subjective ratings of muscle pain during exercise, increase antioxidant action and reduce production of enzymes that are associated with muscle pain after exercise. These authors also found that curcumin ingestion could increase muscular performance by inhibiting inflammation in joints thus improving range of motion and mobility during maximal contractions. Overall, these authors concluded that there was strong evidence that supplementation with curcumin produced reduced markers of both oxidative and mechanical exercise damage in muscle, reduced inflammation (particularly in joints), improved range of motion, mobility and repeated muscular effort (through reduction in discomfort levels).
In terms of how much curcumin to ingest, Nanvati et al (2022) suggest curcumin is a challenging substance to suggest. This is because curcumin has poor bioavailability and metabolises poorly in the intestine and liver. Consuming curcumin alongside black pepper seems to be the best way to increase its absorption into the body (although new supplements are being developed that contain absorption enhancing properties). To elicit the recovery benefits of curcumin, supplementation immediately after exercise appears best. Nanvati et al (2022) suggest 400-1000mg of curcumin once or twice a day appears ideal to improve muscle performance and recovery, however some studies have reported ingestion of up to 5000mg a day for optimal recovery benefits. 180mg of curcumin 2 hours before or after exercise may be enough to elicit antioxidant benefits.
To achieve these levels will require supplementation as pure Turmeric powder is only 3-6% curcumin. This means that a teaspoon of turmeric powder only contains 200mg of curcumin. That would require multiple teaspoons in one meal to get the desired effect.
It would appear that the hype surrounding the use of many of these supplements (or “superfoods”) is largely unwarranted. While minor enhancements have been reported for exercise performance, the main benefit appears to be for post-exercise recovery with anti-inflammation properties being most supported. That said, the evidence isn’t strong, or consistent and the amounts required to elicit beneficial responses are often far more than could be obtained from food itself. Given that the effects appear limited, and the considerable cost associated cost of purchasing all of these in supplement form, it would be difficult at this stage to build a strong case for recommending many of these to a client.
Of all of the items discussed, only curcumin appeared to produce strong and consistent evidence of benefit to athletic populations. Every other nutrient showed tendencies towards benefit, but the authors of each review concluded by saying more research needs to be done before the benefits often reported in the marketing of these products can be substantiated. Many of the reported benefits were subjective measures (i.e. based on athlete perception) which can still make them beneficial for performance. If an athlete perceives less discomfort during exercise, they are likely to complete more work.
The good news is, that the consumption of the above products did not result in any negative effects on performance, so if an athlete was tempted to try one of these approaches, there is little harm in that. It must also be remembered that all of these products do have evidence-based research to support their use in supporting good health (rather than performance), so may still offer benefits for athletic populations.
You now have a greater depth of understanding of common supplements and the evidence-based research associated with each. This information should give you the confidence to have discussions with your clients about these if they approach you about them and give you the ability to answer any questions they might have. That said, it is important that we recognise our professional boundaries when it comes to recommending a supplement to a client. This requires another level of knowledge that involves knowing how each of these supplements might interact with any prescribed medication the client is on, or how they might affect any health complaints or conditions they suffer from. This level of knowledge falls outside our scope of practice, so every personal trainer should have referral pathways to link their clients to industry professionals who are qualified to recommend supplements.
The following is a reminder of the different roles in the field of nutrition and the services they can offer any clients you refer to:
Nutritionists
Remember, the term Nutritionist is not protected. Therefore, anyone with even a little bit of nutrition knowledge can call themselves a “Nutritionist”. Only Dietitians can work as nutritionists in hospitals or other settings that provide nutritional assessment and counselling.
Nutritionists versus registered and associate registered nutritionists
A nutritionist has usually completed a degree in Human Nutrition or related Science, has relevant tertiary training, and has experience in the field of nutrition. However, not all nutritionists meet this criterion, which is why it is important to seek the advice of a Registered or Associate Registered Nutritionist.
Registered nutritionists have met the criteria determined by the Nutrition Society of NZ and can work in areas such as:
- Public health promotion.
- Sports nutrition.
- Research.
- Teaching.
A Registered Nutritionist must hold a degree or academic qualification from a university or other recognised national institution of education. In addition to their basic academic qualification, they must have 2-3 years of professional experience in the field of nutrition. The selection process is overseen by the Nutrition Registration Panel which is an expert group of Nutrition Society members representing academia, industry, government, and private practice.
Registered Nutritionists can work in a diverse range of settings. Registered Nutritionists work within their specific fields of expertise (as determined by the Nutrition Registration Panel), adhere to The Royal Society of New Zealand Code of Professional Standards and Ethics and must participate in a Continuing Education Competency Programme. The title of Registered Nutritionist can only be used by those who meet the standards determined by The Nutrition Society of New Zealand.
Dieticians
A Dietitian is a registered health professional who meets the standards of professionalism required by the New Zealand Dietitians Board under the Health Practitioners Competence Assurance Act. Dieticians have an accredited undergraduate science degree in human nutrition and a post-graduate qualification in Dietetics. Dietitians are trained in the science of nutrition and diet therapy and qualified to work in areas that require nutritional assessment and counselling.
A Dietitian or Registered Nutritionist may work in a variety of settings ranging from Government, community, public health, sports, research and education and the food industry. Dietitians may also work in hospitals.' (Nutrition Society of New Zealand, n.d.)
Either of these referral pathways would be appropriate for a client seeking advice on whether or not to take a dietary supplement. If the desired effect of supplementation is to enhance performance, then a registered nutritionist or dietician that works in sports performance settings would be the best option. If supplementation was to elicit a specific health effect, or a client has a particular medical issue requiring prescription medications, then encouraging them to go through their GP is the best course of action.
Right, time to apply what you have learned. Head to your assessment for an assessment guide video and instructions on submitting your assessments. This assessment will require you to apply the knowledge you have learned and practised by completing a case study relating to micro-nutrient and supplementation.
The assessment guide video explains your assessment task in detail, which requires you to use the information you have learned on this topic to help a case study client.
