The skeletal system is a vital framework that provides structure and support to the human body, allowing for movement, protection of organs, and production of blood cells. Understanding the skeletal system requires knowledge of the bones, joints, and connective tissues that compose it, along with their specific roles and characteristics.
In this online learning session, you will recap the information covered in your face-to face lessons on the topic of bones. You will also be introduced to some new learning material as we dive deeper into how bones grow and are maintained over our lifecycle.
Enjoy your online learning session. Remember to make notes about anything that you are unsure of, so you can clarify these points with your tutor during your next face-to-face session.

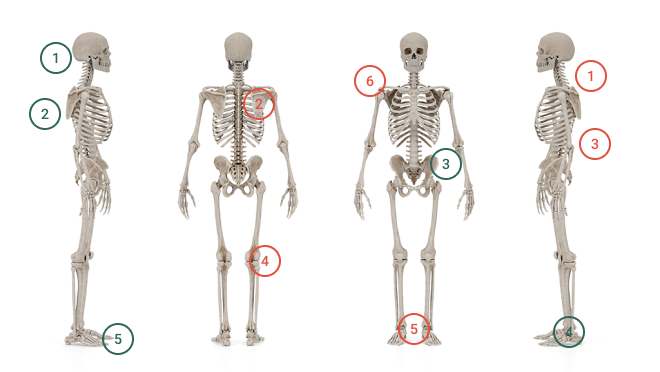
It is important that you can identify the main bones of the human skeleton. We will use these in later topics as we discuss joints, muscle attachments and injury prevention and rehabilitation.
While an adult skeleton has 206 bones, there are 25 main bones (or groups of bones) that you should be able to identify the location of at this level of study. We have covered most of these in our face-to-face class this week. One area of the body we will focus on a lot in later parts of the course is the spine. Let’s take a closer look at the spine now.
The Spine
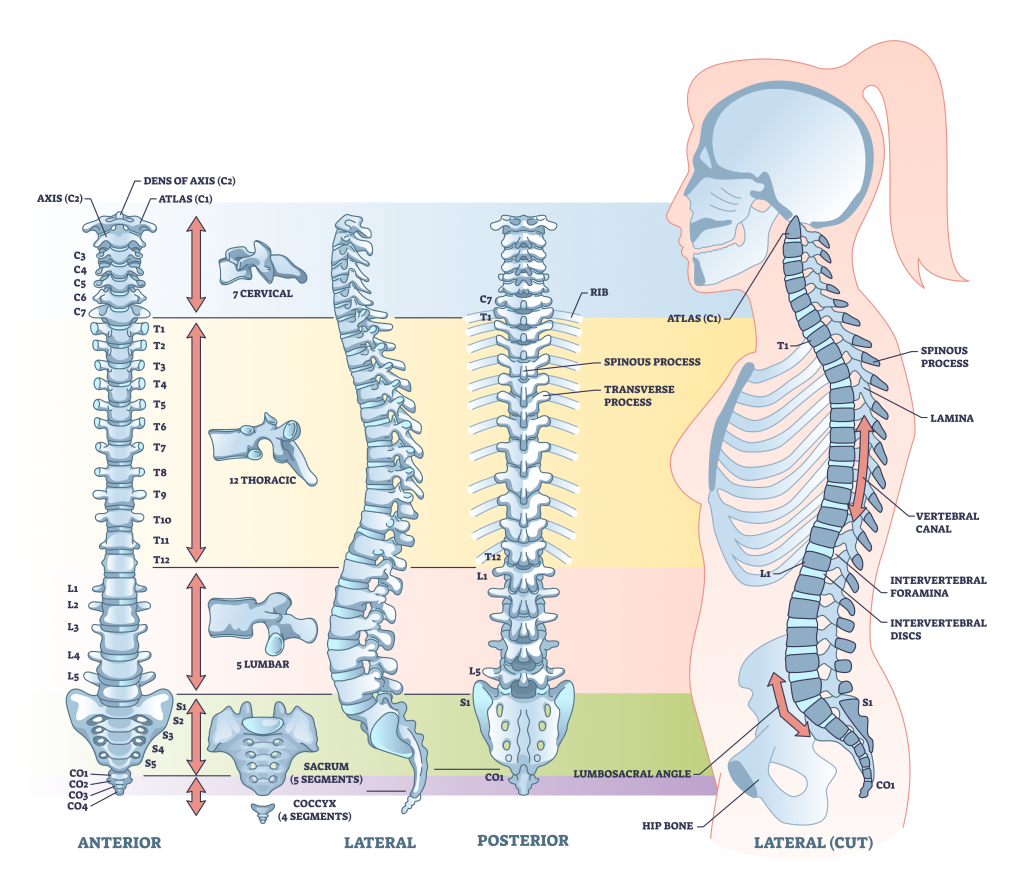
The spinal column is composed of 33 independent bones referred to as vertebrae. These vertebrae are divided into five sections where the structure of each vertebra is slightly different due to the functions each performs. The vertebrae are held together by a strong network of ligaments and cushioned by vertebral disks.
Each of the following regions of the vertebral column has a specific number of vertebrae. Each is attributed a letter (representing the region) and a number (listed from top to bottom in the region).
- The Cervical Spine
- Makes up the neck. There are 7 cervical vertebrae, from C1 that articulates with the back of the skull, to C7 (at the base of the neck).
- The Thoracic Spine
- Aligns with the ribs in the thoracic cavity. There are 12 thoracic vertebrae, from T1 that accepts the first ribs, to T12 (at the base of the ribcage).
- The Lumbar Spine
- Makes up the lower back. There are 5 large lumbar vertebrae, from L1 at the top of the lower back, to L5 (which connects to the sacrum).
- The Sacrum
- The sacrum consists of 5 fused sacral vertebrae. S1 joins with L5, while S5 attaches to the coccyx.
- The Coccyx
- The coccyx consists of 4 fused coccygeal vertebrae (CO1-CO4) which make up the tailbone.
This short video will give you a visual overview of the 5 regions of the spinal column.
This video gives a visual overview of the 5 regions of the spinal column
- Post Watch Task: Considering the structure of the spinal column you have just seen (and what you know of your own spine) answer the following question.
Considering the structure of the spinal column you have just seen (and what you know of your own spine) answer the following question.
H5P here
The task below assesses your ability to identify the main bones. Each question will ask you to identify a selection of bones that are numbered on the image. Attempt this task as many times as it takes until you can consistently identify the correct bones on each slide.
H5P here
Ready for a challenge?
Let’s see how good you are at remembering bone locations under pressure! This is an Anatomy Arcade game called “Whack-a-Bone”. This game is a great place to apply your current knowledge of bone location. There are also a few additional bones and bone regions (like the spine) included in the game that will help you continue to expand your ability to locate bones. If you are new to this app, you will have to start in the middle of the “map”. Once you complete the Whack-a-Bone” challenge you can progress to some higher-level challenges.
This week you should spend a minimum of 15-20 minutes honing your skills on this app. You can then revisit the link in the future to keep your skills sharp and expand your knowledge even further.
Feel free to post a screen shot of the stage you get to this week to the Teams chat. See if you can further than your classmates this week.
What is bone?
There are some key structures that form bone and give it both strength and flexibility. Can you identify the two key components of bone?
H5P here
Bone Shapes
Bone forms into various shapes which are designed for specific functions. There are 5 classifications for bone shape:
- Long
- Short
- Flat
- Irregular
- Sesamoid
The following tasks assesses your ability to identify the shape (classification) of bones. Each card has a image of a bone (or bones). For each image, enter the shape classification you believe the bone (bones) belongs to.
The functions of bone
The shape of a bone aligns with its function in the body. The following task tests your awareness of the different roles of bones (linked to their shape). Feel free to read over your course notes before attempting these tasks.
H5P here
Bone types
Earlier in the week we learned that there were there are two main types of bone. The following task checks your ability to recall these bone types and the details for each that we covered in class. Feel free to have a quick read over this information in your learner resource before attempting this task.
H5P here
The Lifecycle of Bone
This week, we learned that there are some differences in the way that males and females grow and maintain bone across their lifecycle. Take a moment to study the image below before answering the questions that follow.
The Lifecycle of Bone

Below is a short series of multi-choice questions relating to the image above.
H5P here
This next activity helps explain the two main ways in which bone grows.
H5P here
The Cells Involved in Bone Formation
- Osteogenic Cells – these are stem cells from which the other two key bone cells are made.
- Osteoblasts – these are bone making cells that build new bone matrix (collagen) for minerals to layer upon.
- Osteocytes – these are actual bone cells. They are osteoblasts that have become trapped by minerals and are now part of the bone tissue. Once formed, these cells actively monitor bone and assist in maintaining mineral balance between the bone and blood.
The Cells Involved in Bone Formation
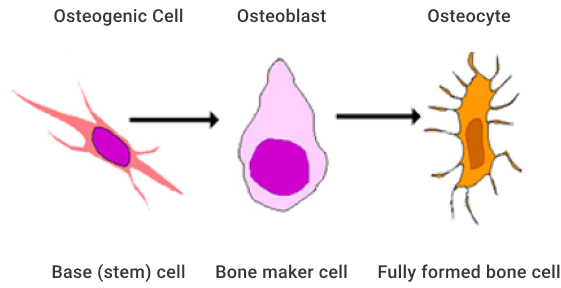
In summary, osteogenic cells form osteoblasts. Osteoblasts lay down new bone matrix (collagen). The blood then brings minerals to cover the base collagen. This mineral deposit traps the osteoblast forming a new bone cell (or osteocyte). The osteocytes continue to monitor the bone and assist the exchange of minerals in the blood to ensure mineral levels throughout the body are maintained.
This video provides an in depth look at bone biology. It gives you some great insights into the two main types of bone (compact & spongy), the role of osteocytes within bone, and the role of bone marrow.
Learn the basics of bone biology, including the different elements that make up bone and how those pieces work together, in this short and visually dynamic animation.
Source: YouTube
Bone is Not a Constant Entity
Did you know that your bones are constantly changing?
During childhood and adolescence bones are formed through a process called modeling. This is largely driven by rising levels of sex hormones (testosterone and estrogen). This is a period where major bone growth occurs (both in length and density). But that’s not where changes to bone end.
In fact, around 10% of your bone tissue is renewed every year. This means that most of the adult skeleton is replaced about every 10 years! (Bone Health and Osteoporosis: A Report of the Surgeon General, 2004).
There is constant cellular activity within bones. Bone matrix is continually being broken down and reformed. This process is called remodeling. The bones contain significant stores of minerals. These are required throughout the body for a range of bodily functions. Osteocytes within the bones work with blood, to ensure blood levels of these key minerals are maintained. Provided nutritional intake is sufficient, new mineralisation of bones will occur shortly after.
We have already established that cells known as osteoblasts lay down new bone matrix (collagen). We also know that some become trapped within the bone by the minerals that are laid down in the bone forming process. But how do bones get broken down in the remodeling process?
This video allows you to take a look at this amazing process in action and the work that is done by the tiny cells that facilitate bone growth and change. It also discusses some of the lifestyle factors that can drive each of these key cells to be more active in their role leading to increases or decreases in bone density. Watch the video and take some notes at the back of your learner resource. This will help you to answer the questions that follow.
Bone Remodeling and Modeling
This video illustrates the processes of bone remodeling and modeling over time using high quality animation.
- Pre watch task: Watch the video and take some notes at the back of your learner resource. This will help you to answer the questions that follow.
- Post watch task: Answer the short series of questions that follow the video.
Source: YouTube
The questions in the task below relate to the content covered in the video above.
As we discussed in class, there are three key factors that have the largest influence on bone growth:
- Sex hormone levels: Testosterone and estrogen (along with other hormones) stimulate bone deposits. The secretion of these hormones peaks through the later stages of puberty and remain elevated until our early 20s, then gradually reduce as we age.
- Nutritional intake: Adequate food intake (especially protein) is important for the maintenance and growth of bone, as is a regular consumption of key minerals.
- Exercise and Activity (amount and type): The best exercise to stimulate bone growth and maintenance is loaded exercise. This refers to regular activity that places repetitive stress on bones to encourage bones to adapt (strengthen). Our levels of this kind of exercise usually decline with age.
Let’s look at each of these in a little more detail.
The Role of Hormones in Bone Development and Maintenance

Sex hormones, particularly estrogen and testosterone, play crucial roles in bone growth and maintenance throughout the human lifecycle. Their influence begins in childhood, peaks during adolescence, and continues to affect bone health into adulthood and old age.
During childhood and adolescence estrogen and testosterone both contribute to the growth spurt during puberty by stimulating the growth of long bones. Testosterone in males and estrogen in females promote the action of osteoblasts, which are responsible for adding new bone tissue, leading to increased bone length and density.
In adulthood, the sex hormones are crucial for maintaining bone density. Estrogen helps to prevent bone breakdown by inhibiting the activity of osteoclasts and testosterone continues to promote osteoblast activity.
A healthy balance between bone formation (by osteoblasts) and bone breakdown (by osteoclasts) is largely maintained by adequate levels of sex hormones. This balance ensures that bones remain strong and dense.
Hormones as We Age
As we age, the secretion of sex hormones starts to decrease. In females, the process of menopause causes a significant drop in estrogen which sees osteoclast activity increase, thus accelerating bone breakdown. This continues after menopause, which is why post-menopausal women are at higher risk of developing bone density issues. Testosterone secretion also gradually decreases in men, but the process is slower, so the effects of bone density reduction are less significant. This can be seen in the image below.
| Changes of Hormone Estrogen Levels in Female | |
|---|---|
| Estrogen Hormone Level | 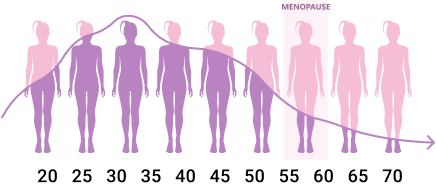 |
| Changes of Hormone Testosterone Levels in Male | |
| Testosterone Hormone Level | 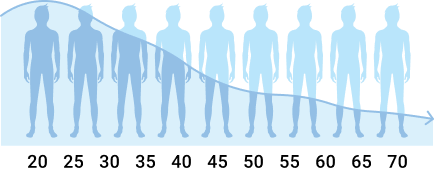 |
Of course, other factors can also impact on hormonal levels such as genetics, hormonal disorders and certain medications. In short, if hormonal levels are affected, then the remodelling process of bone will be also.
The Role of Nutrition in Bone Development and Maintenance
Bone can only be formed if the nutrient building blocks are available. The key nutrients that play a role in bone health include:
The main ones:
- Calcium
- Vitamin D
- Protein
The secondary ones:
- Magnesium
- Phosphorus
- Potassium
- Boron
- Vitamin K2
If you eat a healthy diet with lots of fruits, vegetables, legumes, nuts, seeds, and lean proteins, you’ll get enough of most nutrients needed to keep your bones healthy and functioning well. Of course, some dairy, or dairy replacement foods are important too!
This short video provides some great food ideas for including in your diet to ensure bone health is maintained. Some of them you will already know benefit bone health (e.g. milk and other dairy products) but others you might not have realized have bone benefits. Jot some of these down at the back of your learner resource for future reference. The video moves through the foods quickly, so hit the pause button at intervals to ensure you get a good number written down.
Serve Up Bone Strength - preventing osteoporosis through nutrition
Getting the right nutrients to build and strengthen your bones may be easier than you think! This short video highlights a bunch of foods that you can include in your diet regularly to ensure good bone health.
- Pre watch task: Write some of the food ideas this video shares in the back of your learner resource for future reference. The video moves through the foods quickly, so hit the pause button at intervals to ensure you get a good number written down.
Source: YouTube
The Role of Exercise in Bone Development and Maintenance
Our learning in class has already established the importance of “loaded exercise” in maintaining adequate levels of bone density throughout adulthood. Now that we know more about the cells involved in the bone modeling and remodeling process, we can better understand the process by which activity leads to better bone density.
Loaded exercise places mechanical stress onto our bones. Bones can actually bend slightly during loaded exercises like running. In fact, your bones are subjected to a range of forces during loaded exercise including compressive forces (from weight bearing down with gravity), tensile forces (as muscles pull on the bones they are attached to), and shear forces (as bones move against each other). The image below shows how these different forces acting on the foot and ankle during running lead to a slight bending of the bones.
Bone Bending Under Stress
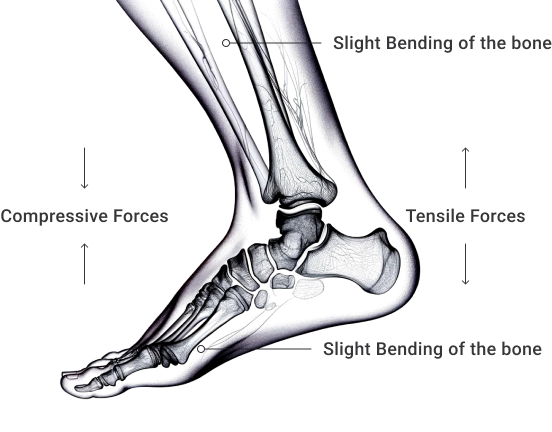
This bending (stress) of bones alerts the osteocytes within bone which act as sensors. When osteocytes sense this stress, they send signals to osteoblasts which activate and begin laying down new bone tissue to reinforce the bone at the sites where the stress was applied. Through repeated application of stress, this remodeling leads to an overall increase in bone density.
It is worth noting that the areas of bone that experience the most stress will be the areas where bone density is improved, so effects can be quite site-specific, for example, an exercise like squatting would elicit bone density gains in the spine, hips and lower limbs, while an overhead shoulder press will improve bone density more in the upper limbs.
As people age, they tend to do less loaded exercise. This is another factor that contributes to a reduction in bone density with age.
Answer this series of questions to check your understanding of the new information we have covered in this online lesson. Included in this recap task are also questions related to the bone density and exercise content we covered in this week’s face to face classes. Feel free to read over that content again before attempting these tasks.
There are a number of common bone related issues that you may come across during a role in the sport, recreation and exercise industry. These can be broken into acute (one-off) and chronic (long-term) conditions.
The most common bone related injury is a fracture. Bone fractures range from tiny cracks in the outer layer of a bone (compact bone), through to complete breaks (where a bone is separated into pieces (or shattered). Fracture treatment is the domain of medical professionals. But there are a couple of pieces of information related to bone fractures that are worth noting for a role in the sport, recreation and exercise industry.
The two population groups that are most susceptible to bone fractures are children and older people.
Children and Fractures

According to Hedstrom et al (2010), nearly 40% of children will experience at least one fracture before the age of 17. Children are more susceptible to bone fractures for several reasons:
H5P here
Older people and fractures

Around 50% of women and 20% of men over 50 will experience at least one bone density related fracture in their lifetime (Coughlan & Dockery, 2014). Older people are more susceptible to bone fractures due to several key factors related to aging and changes in bone structure.
H5P here
Considerations for exercise selection
When selecting exercises for people with compromised bone density there a couple of key considerations:
- Reduce strain velocity to reduce impact - Exercise selection should focus on magnitude (loading) and frequency.
- Ensure points of contact – Due to the factors mentioned above, it is imperative that we reduce fall risk during exercise. At least two points of contact should be maintained during all exercises (i.e. feet on floor, hand on rail or wall).
Stress fractures
Stress fractures occur due to repetitive, cumulative stress on the bones, typically from overuse in activities like running, jumping, or sports. Unlike fractures caused by a single event, stress fractures develop gradually when the bones are subjected to repeated mechanical loading without sufficient rest.
This video outlines what a stress fracture is along with their common causes.
Stress Fractures in Athletes Part 1 – Identifying Causes and At-home Treatment
This video explains explains what stress fractures are, how they happen and at-home care options.
Source: YouTube
Stress fractures are particularly common in active adolescents. Here’s why.
H5P here
Recap of new Learning
The following short quiz is designed to test your retention of the content you have just covered.
H5P here
The following content is designed to recap on the key learning you have covered in face-to-face classes this week. For this reason, these recap tasks should be attempted only once the joints topic has been completed in class.
In between the recap activities, there is some new content for you to consider. If anything in this new content leaves you confused or wanting to know more, note down any questions you have and bring them into your next face-to-face class where you can clarify your understanding with your tutor.
This short series of questions will check your understanding of joint structure and function. Feel free to read over the course notes in your learner resource before attempting the questions.
As we established in class, joints have different physical structures that predispose them to being designed either more for stability or more for mobility. For example, the upper vertebrae of the neck are designed for mobility, while the lower cervical vertebrae are designed for stability (i.e., holding your head in position above the torso and providing a stable base for upper cervical movements).
The video below describes these movements in the neck. While you are watching the movements, note the differences in mobility between the upper and lower regions of the cervical spine.
Human Anatomy Explained: The ultimate guide of cervical spine movements
This video explores the range of motion, and movements performed at the cervical spine. It reviews the flexion, extension, lateral flexion, and axial rotation of the neck.
- Pre watch task: While you are watching the movements, note the differences in mobility between the upper and lower regions of the cervical spine.
Source: YouTube
You can see from the images below that the first 2 cervical spine are designed specifically for their role. The C1 vertebra has two small sockets for the base of the skull to rest on. The joint between the skull and the occipital bone (back of skull) is a hinge joint which facilitates most of the flexion and extension of the neck. The C2 vertebra has a boney projection called the “dens” which allows the C2 to rotate against the C1 leading to neck rotation.
Atlas and Axis

Stability or mobility?
While synovial joints are classified as “freely movable”, each joint has a tendency towards providing stability or mobility.
The image below shows how joints can be categorised using this concept. As you can see, the upper neck, shoulders, hips and ankles are primarily designed for mobility, while the lower back, knees and feet are mostly there for stability (but of course still offer movement).
Joint by Joint Concept
| Mobility | Stability |
|---|---|
|
|
Misalignment and Imbalance
In many joints there needs to be a happy medium between stability and mobility for proper function. For example, if an ankle was to become excessively mobile, it would likely increase the risk of injury. Similarly, if the lumbar spine becomes excessively stable (stiff), the body may recruit movement from other areas of the body to compensate. These areas may not be designed to carry load and could become prone to injury also. These compensatory areas will also recruit different musculature which could lead to an unwanted muscle imbalance.
Misalignments and imbalances are common and can arise due to a variety of reasons including genetics, the environment we live in, the activities we choose to do often, and injury.
Let’s briefly explore each of these causal factors.
Genetics
Some of us are just born different! Skeletal structure can be something you inherit from your elders. The width of your hips, the curvature of your spine, the length of your bones and the angle at which your bones insert into your joints can all be influenced by your genetic make-up.
Check out the different frames each of these athlete’s exhibit in these photos from Howard Schaltz’s 2002 book “Athlete”. While they have undoubtedly trained hard to be good at their sport, you can tell that they were given certain genetic traits that assist them in their sport.
Wilkinson and Zeggini (2021) suggest that while genetics can affect joint structures across the body, the hip and pelvis are the most common site for established genetic variation in joint shape.
Given the location of the hip and the load bearing nature of the joint, the associated effects of this genetic differences can have wide ranging effects on other joint alignments in the body. However, it is extremely difficult to counter genetic issues with exercise.
The image below shows how people’s femurs can insert into the pelvis at different angles. Slight differences in bone angle at the joint along with different shapes and depths of socket, can lead to drastic differences in mobility and stability of the joint (this explains why some people can do the splits!).
Femur Insertion Angles
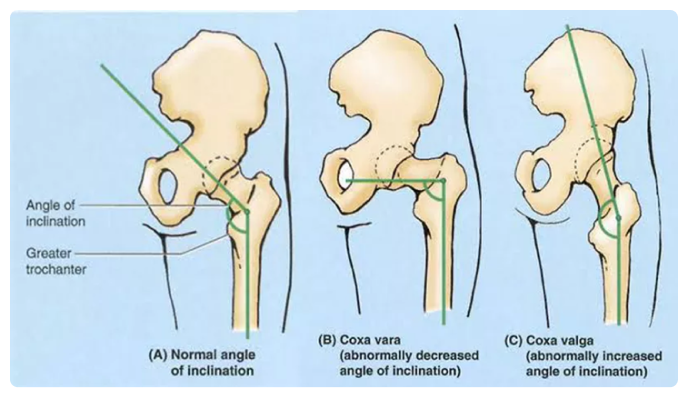
Image sourced from https://medizzy.com/feed/23373456.
The environment
Modern living sees us sitting more than we ever have before. Not only are we sitting, but we are also engaging with technology far more than previous generations. Whether this be for work or enjoyment, the amount we are sitting (and the way we are sitting) is having an undeniable effect on our body alignment. This factor can also be related to the furniture or equipment we use regularly. For example, someone who has a low workbench or countertop may adopt a stoop like stance, while some sofas and chairs may encourage a less-than-optimal sitting position (e.g. La-Z-boy chairs or reclining sofas).
Repeated activity
The nature of a person’s job or the sport or activity that they regularly play may also result in imbalances that can affect their posture. For example, hockey players are often bent forward over the ball. One-limb dominant athletes like tennis players or baseball pitchers will create imbalances between the dominant and non-dominant sides of their bodies. Courier and truck drivers spend the best part of their day sitting which can lead to chronic shortening of muscles and other workers involved in repetitive tasks are likely to develop imbalances, e.g. someone who works a shovel all day.
Injury
There are a number of injuries that could affect joint stability. The most common of these affect the ligaments of the joint. In your face-to-face classes this week you were introduced to three common ligament related injuries. Let’s see what you remember about these.
H5P here
Structural vs Functional Issues
As you can see, there are a number of factors that could lead to joint misalignment or muscle imbalance. Issues can typically be categorised as structural or functional.
These terms help categorise body alignment issues so we can best determine how we can ( or if we should) attempt to correct them.
Structural issues refer to those issues that are simply present due to the way your skeleton has developed. These are often genetic issues that are to do with your bone shape and joint structure. Trying to correct these issues through exercise may cause additional problems as you try to force a change that simply can’t happen.
Scoliosis of the spine is a structural issue
Functional issues are those that relate to muscular imbalances. These have usually either come about through your daily behaviours or lifestyle (work - see image #1 and relaxation), the environment you live in, or the type of physical activity you have performed (e.g., a cyclist bent over the handlebars for thousands of hours of training - see image #2). These alignment issues are usually muscular in nature, i.e., some muscles have tightened over time while others have weakened. Functional issues are usually able to be corrected with targeted exercise.
Let’s put this is a practical sport, recreation and exercise context. Imagine you are working with a new PT client in the gym. You ask them to perform a back squat with just the bar, and this is what they manage to do.
Obviously, something is not right here, but is it a structural issue that stops this client from keeping a straight back while squatting (e.g., tight lower back, hamstrings or calves) - see image #3 (https://startingstrength.com/training/when-to-do-the-lifts-wrong), or do they have a structural issue like deep hip sockets causing the problem?
Recap of new learning
This short quiz will see how well you have taken on board the information we have just covered. Feel free to read over the notes again before attempting these questions.
H5P here
Human body movements are facilitated by co-ordinated joint movements. While these movements are initiated and monitored by the nervous system (and produced by the muscular system), the movements themselves are guided by the structure of the joints (and the way that the muscles attach to them).
By learning the movements possible at each joint, along with the muscles responsible for generating the movement, you are in a better place to understand how to train to enhance the strength, power and endurance of these movements. This knowledge is key to being able to produce targeted and effective programming for muscle function development.
The following recap task is a flash card task assessing your recall of joint movement types. Look at the image on each card, then type in the movement you believe it is. The joint the movement is occurring at has been provided, you only need to answer with the movement term.
H5P here
Joint movements related to gym exercise
Knowing the joint movements is the first step in understanding the gym programming process. The next step is to be able to recognise these movements in common exercises. First you must identify the joints involved in the movement. Then you can identify the movement at each joint. Some exercises are isolated (only involve one joint), while others are more complex (compound) and involve multiple joints.
This short series of questions is designed to assess your ability to identify the joint movements within common resistance training exercises. Remember, we are only interested in identifying the joint movement that occurs during the work phase of an exercise (i.e., when the weight is lifted, or a person works against gravity in a body weight exercise).
H5P here
Ensuring muscle balance in exercise programming
Knowledge of joint movements is also the first step in ensuring you create exercise programs that will ensure muscle balance. As we have already discussed, many people exhibit muscle imbalances that are brought on through the way they live and the activities they do regularly (e.g., work, sport etc.).
Muscle balance in an exercise program is achieved through careful consideration of exercise selection to ensure the muscles acting on both sides of a joint are targeted equally. This is where knowledge of joint movements comes in handy. Without even knowing the muscles that different exercises target (don’t worry, you will learn these), you can still ensure you select exercises that will achieve muscle balance.
All you have to do is:
- Select an exercise
- Identify the joint movements involved in the exercise
- Identify the opposite joint movements to those used in the exercise
- Select an exercise that uses these joint movements.
An example:
| First exercise selected: | Bench press |
| Joint movements involved: | Horizontal adduction of the shoulder, elbow extension |
| Opposite movements: | Horizontal abduction of the shoulder, elbow flexion |
| Exercise that uses those movements: | Wide Grip Seated row |
If a person has an existing imbalance, a program will have to be constructed that targets the imbalance. This involves identifying the muscles that are tight and releasing them (approaches like stretching and foam rolling are good for this) and identifying the muscles that are weak (or not recruiting properly) and targeting them with exercises. We will explore this concept in more detail in the muscle topic of this module, and again during our exercise prescription modules.
End of Topic
That’s topic 2 done and dusted. Hopefully you feel you have a good understanding of bone location, type, growth and development and common issues related to bones. We have also covered the different types of joints and started the process of learning key joint movements that are involved in exercise. We will build on this knowledge in the upcoming muscles topic, and also during our first Exercise Prescription module later in the semester. Next, we will learn about the system that tells all our other systems what to do. The Nervous System.
