- Reading A: WHS Framework
- Reading B: Guidance for Officers in Exercising Due Diligence
- Reading C: Managing Risks to Health and Safety at the Workplace Fact Sheet
- Reading D: Risk Management Prompt for Hazardous Manual Tasks
- Reading E: Slips and Trips at the Workplace Fact Sheet
- Reading F: Work-Related Stress
- Reading G: Work Stress in Human Services
- Reading H: Sample WHS Consultation Procedures
- Reading I: Organising Health and Safety Training in your Workplace
- Reading J: Record Keeping
- Reading K: Incident Management and Reporting Guidelines
- Reading L: Incident Management and Reporting Guidelines
- Reading M: Benchmarking

The Institutional Framework
To address developments in health and safety, Australia has created an institutional framework involving key players, often with differing interests.
| Key Players | Interests |
|---|---|
| Workers |
|
| Employers |
|
| Governments |
|
| Insurers |
|
| Health and safety professionals: nurses; ergonomists; occupational physicians; hygienists, psychologists, therapists; safety engineers and rehabilitaion providers |
|
In addition to these immediate players are the associations representing workers, such as unions, trade associations, state and territory trades and labour councils, the Australian Council of Trade Unions (ACTU), employers’ peak bodies, such as the Australian Chamber of Commerce and Industry (ACCI) and specific industry associations, and, finally, insurer and health professional bodies. Other players include the courts, lawyers dealing with health and safety and compensation law, standards bodies, scientists carrying out research into hazards and health and safety consultants.
There are also international bodies active in health and safety that governments and others recognise as having a role to play, such as the ILO [International Labour Organization] and the WHO [World Health Organization]. Australia has ratified the ILO’s Convention on Occupational Safety and Health (No. 155), which requires countries to implement a national policy on occupational health and safety in the workplace.
Consultation and Cooperation
The improvement of health and safety depends on a variety of participants cooperating at times when their interests do not always point them in the same direction.
Australia has tried to build consensus among these participants and direct activities towards agreed goals using health and safety legislation and commissions – government supported bodies in which players meet to determine policy and strategy.
Under Australia’s federal system, there are three levels at which players are brought together.
Federal Level
In 2009, Safe Work Australia (SWA) was created to take over from the Australian Safety and Compensation Council (ASCC), which was the successor to the National Occupational Health and Safety Commission (NOHSC).
Safe Work Australia
Safe Work Australia is an Australian Government statutory agency set up to:
- Coordinate and develop national policies and strategies
- Assist with the implementation of model work health and safety legislation and reform the legislative framework
- Undertake research
- Collect, analyse and report data.
It is tripartite and comprises 15 members, including an independent chair, nine members representing the Commonwealth and each state and territory, two representing the interests of workers, two representing the interests of employers and the CEO of Safe Work Australia.
Safe Work Australia overlooks the Australian HS Strategy and was instrumental in harmonising law using the Model WHS Act. SWA collects health and safety statistic, the National Data Set. Its annual report, Compendium of Workers’ Compensation Statistics Australia, gives an overview of health and safety in Australia, showing trends based on accepted workers’ compensation claims.
SWA is not a regulatory authority. It does not pass or enforce laws. Health and safety laws in Australia operate in each of the state, territory and Commonwealth jurisdictions, and are administered by jurisdictions’ regulators.
Two other bodies need mentioning – the National Industrial Chemicals Notification and Assessment Scheme and the Federal Safety Commissioner.
The National Industrial Chemicals Notification and Assessment Scheme (NICNAS)
The Australian Government’s industrial chemical safety regulator, the National Industrial Chemicals Notification and Assessment Scheme (NICNAS), was established in 1990. NICNAS provides a national notification and assessment scheme to protect the health of the public, workers and the environment from the harmful effect of industrial chemicals. It assesses all chemicals new to Australia and assesses those chemicals already used (existing chemicals) on a priority basis, in response to concerns about their safety on health and environmental grounds.
NICNAS produces assessment reports that contain safety recommendations for the handling and labelling of the chemical. It also publishes the Chemical Gazette electronically every month and the Australian Inventory of Chemical Substances (AICS), which lists more than 38 000 chemicals. The latter is a very useful free online database.
Office of the Federal Safety Commissioner
In 2005, a Federal Safety Commissioner (FSC) was appointed to the then Department of Employment and Workplace Relations. The functions of the FSC include:
- Promotion of best-practice health and safety on Australian Government building and construction projects
- Development and administration of the Australian Government Building and Construction OHS Accreditation Scheme (now mandatory)
- Promotion of the adoption of safe design on Australian Government construction projects with the aim to eliminate and/or minimise health and safety risk during the construction phase
- Work with industry stakeholders to identify initiatives that will lead to an improved health and safety performance in the industry.
In this role, the FCS provides useful understanding of how to make sure contractors in general, not just construction, manager their HS [health and safety]. Their website contains some excellent resources.
Jurisdictional Level
Because the Constitution does not give the Commonwealth general power to legislate for health and safety, there are nine principal jurisdictions in Australia – eight state and territory and one Commonwealth. Here, we find WHS acts and government regulators whose role it is to administer their legislation; for example, collect incident data, provide information and carry out inspections and prosecutions.
In addition, governments also support the commissions that oversee health and safety matters, including compensation and rehabilitation. Here, policy and strategy are debated. At this jurisdictional level, insurers and others involved in the commissions, including the government, employers and unions are to be found.
Workplace Level
Finally, at the workplace or organisation level, there are employers, workers and, sometimes, union representatives and health and safety professionals meeting on workplace health and safety issues. In larger workplaces or organisations, this also involves health and safety committees (HSCs). We will talk in more detail about HSCs later. Needless to say, it is at the workplace level where we see whether health and safety is successful. It is here we see the final outcome.
The experience of working in this framework over many years has led to a consensus that the critical elements within an organisation determining WHS performance are as follows.
| Commitment | Does senior management make health and safety a priority - planning. funding, training, reporting, etc.? How is this communicated? |
|---|---|
| Consultation | Are workers and their representatives involved in WHS decision making at the earliest stages? Do the consultative arrangements have support? Is WHS communication between managers and workers open and two-way? |
| System | Are there policies and procedures? Is there an effective WHS organisation and program for the systematic identification of hazards and management of risk? Is performance monitored, measured, audited and reviewed to ensure continuous improvement? |
| Culture | Is everyone aware of and sensitive to hazards and risks? Do people talk about health and safety? are they empowered to report hazards? |
All four elements are necessary, as set out in the model in Figure 1.7.

The health and safety system of policies, procedures and practices – the machinery – lies at the core; however, it must be fuelled by active management commitment, a spirit of genuine consultation and a robust health and safety culture.

PART I: Due Diligence – Where to Start and What Does It Mean to You?
Due diligence—in the context of work health and safety—means taking every precaution that is reasonable in the circumstances to protect the health, safety and welfare of all workers and others who could be put at risk from work carried out as part of the business or undertaking. This includes work carried out overseas.
Due diligence is a powerful and proactive management tool that will help to foster the careful and systematic identification and assessment of specific workplace hazards and the establishment of control measures to prevent injuries and illnesses at work.
If you are an officer, due diligence requires you to take reasonable steps to address each of the definition elements for due diligence outlined in section 27 of the WHS Act. Each of the elements is directed at one or more of the elements of a safety culture and the drivers of safe behavior.
The first step requires every person in the workplace to understand and comply with their duties set out in the WHS Act. Due diligence requires officers to be proactive in ensuring that a department, agency, public authority or corporation complies with its duty, including workers working or posted overseas.
The next steps include the need for officers to identify risks to safety, health and welfare in the workplace, including risks identified in the WHS legislation and approved Codes of Practice. Once risks are identified, due diligence requires that you address these risks through a properly functioning and documented health and safety system. The more harmful or serious the potential dangers are, the more you must guard against them to prevent workplace injury and illness. An officer’s due diligence obligations in respect to managing workers overseas are identical to those onshore. Some general measures to comply with the WHS Act and demonstrate due diligence include:
- setting up a well-documented system for identifying, reporting, and responding to all actual and potential hazards in the workplace
- ensuring safe practices, procedures and controls are in place that are specific to the hazards in your workplace that either meet or exceed the requirements set out in the WHS legislation—including relevant approved Codes of Practice
- providing ongoing instruction and training to supervisors, managers and workers
- communicating regularly with workers about foreseeable health and safety hazards
- allocating adequate time and resources for health and safety, including health and safety committees
- monitoring and auditing health and safety programs on a regular basis.
Compliance with each of the elements of due diligence will mean officers have a greater understanding of what is needed to effectively manage health and safety risks. This will enable health and safety to be more readily integrated into broader strategies—permitting a more proactive, rather than reactive approach to be taken.
In complying with each of the elements of the definition of due diligence, officers will demonstrate their interest in health and safety which should have a positive cultural impact (Sherriff, 9). The active involvement of middle managers, supervisors and workers in each of the processes is critical.
PART II: Suggested Approaches, Ideas and Information Aimed at Assisting Officers in Demonstrating a Due Diligence Framework
How Do I Acquire the Information I Need?
As an officer, you must acquire and keep up-to-date knowledge of the work health and safety matters. This can be met through:
- acquiring up-to-date knowledge of the WHS Act, WHS Regulations and approved Codes of Practice
- investigating current industry issues through conferences, seminars, information and awareness sessions
- industry groups, newsletters
- acquiring up-to-date knowledge of work health and safety management principles and practices
- ensuring that work health and safety matters are considered at meetings.
This may include:
- knowledge that is:
- technical—legal obligations
- situational—what is happening and what it means
- strategic—what should the PCBU be doing and why
- from
- senior managers
- subject matter experts
- managers/supervisors
- workers.
Systems of work, including consideration of the resources and other requirements for the work to be done, will be more likely to provide for health and safety if they take into account relevant information. This is aided by input into the decision making process by all who are involved in managing, supervising and undertaking the work. Consultation obligations in the WHS legislation, including the relevant Codes of Practice are aimed at ensuring that contribution of information.
Ideally, the flow of information should be a continuous process, with information volunteered rather than only provided when it is sought during formal consultation and incident reporting processes.
Information then needs to be:
- gathered
- analysed
- reported.
This can be met by:
- developing a plan of the operations that identifies hazards in core activities
- ensuring that information is readily available to other officers and workers about procedures to ensure the safety of specific operations that pose health and safety risks in the workplace
- continuously improving the safety management system.
Do I Confidently Understand the Risks and Hazards of The Business or Undertaking? Why Do What We Do?
There may be times when the officer’s knowledge of work health and safety and the circumstances in their workplace mean that further expertise may be required to control the risks. For example:
- during periodic reviews of operations of the business
- when developing and implementing systems for the long term management of work health and safety
- when planning to modify the work premises, plant, substances or materials for use at work • before introducing changes to work practices and systems of work
- when establishing new operations or projects
- when a hazardous exposure or incident, injury or illness etc. indicates that risk control measures are inadequate
- when managing complex issues related to psychological health such as bullying and stress
- when working overseas.
Officers may meet the due diligence requirements in some respects by proper reliance on information from, and on the activities of others, while having more direct involvement in health and safety managements and governance in other aspects.
To the extent to which an officer does seek to rely on others, the officer must be able to demonstrate the reasonableness of that reliance, which may be demonstrated through the receipt of credible information and advice from appropriate people.
Officer Considerations
As an officer you should consider whether:
- the right structure is in place for the business or undertaking
- the right people are in the right place
- there are effective means for information flow and advice
- the right information is available at the right time
- there is a proactive as well as responsive approach to managing work health and safety
- there is clear designation of responsibility and accountability
- there is system for regular verification and correction of work health and safety policies and practices
- there is active engagement across the organisation regarding health and safety matters—lead from the top.
An officer may not be exercising due diligence if he or she accepts or does not respond to work health and safety incidents or concerns. If an individual lacks the authority to fix a problem, that individual should escalate information regarding that problem in a timely manner to those who are in a position to fix it. Example—action to ensure that significant issues with the health and safety performance of a contractor, of which they are aware, is properly addressed. Due diligence requires taking positive action to solve problems and manage hazards. Don’t just report it if you have the ability and authority to fix it.
How Do We Protect Our Health and Safety?
A key element for you to consider in meeting your due diligence obligations, is risk management and ensuring there are appropriate processes for receiving and considering information regarding incidents, hazards and risks and responding in a timely way to that information. This can be met by:
- establishing/maintaining safe methods of work
- implementing a safety management system
- ensuring appropriate resources for health and safety are available and used.
Manage The Risk
Risk management is an integral part of good management practice and an essential part of good corporate governance. In order for WHS risk management to be effective, it should be part of an organisation’s culture. Ideally WHS risk management should not be seen as a separate activity. Rather, it should be embedded in an organisation’s processes and practices. Refer to the Safe Work Australia guide—How to manage work health and safety risks for further information on managing health and safety risks.
Risk management is an important part of any health and safety prevention program and the success of such programs depends on successful implementation of risk management.
To exercise due diligence, officers must develop, implement and review a safety management plan to identify possible workplace hazards and carry out the appropriate corrective action to prevent accidents or injuries arising from these hazards.
Hazard identification, risk assessment and risk control at workplace level may be defined as the systematic application of management policies, procedures and practices to the four-step process of:
- identifying hazards
- assessing and analysing the risks
- controlling the risks
- monitoring and reviewing the risk management process.
Are there effective controls in place?
- How do you know if all hazards and risks have been identified and assessed?
- Are risks controlled using all reasonably practicable means?
- Have you evaluated any residual risk?
- Have all systems, policies and procedures been effectively implemented that apply to the operations of the business or undertaking?
- What technology is in place for work health and safety, is it sufficient, does it need updating or reviewing?
- How effective are the controls? Have they been tested?
The benefits of appropriate resources and processes to eliminate or minimize risks include:
- workers, middle and senior management have a heightened awareness of risks within their work environment
- risks are identified, assessed and controlled in accordance with the legislative requirements of the WHS Act
- risk management becomes a part of the organisational and corporate culture
- a reduction in the severity and incidence of workers’ compensation claims, leading to a reduction in associated premiums and hidden costs (such as loss of worker morale, loss of productivity, etc)
- costs of replacing absent injured workers and the loss of productivity.
Elements To Consider in Exercising Due Diligence
As an officer you should be aware that existing corporate governance structures and processes may not meet due diligence requirements under the WHS Act.
You should ensure there is:
- an appropriate structure, with clear charters and key performance indicators to provide for effective communication and accountabilities
- reporting processes for timely, accurate information to officers
- processes in place to provide confidence as well as accurate, up-to-date reliable information about health and safety matters to meet duties and obligations under the WHS Act
- means for ongoing advice and decision making (delegations)
- auditing and other processes for verification of compliance
- documentation demonstrating due diligence activities
Do You Know Your Business And People?
What is your organisational structure e.g. leadership team and worker demographics?
- Who are the management team—what are their strengths, weaknesses and skills in managing risk?
- Have you assigned appropriate accountability to authorized and skilled delegates?
- Do you know your business operating risks?
- Do you understand the activities you have substantial influence or control over for the whole or substantial part of the business or undertaking?
- What other influences may impact on work health and safety—for example financial, safety culture, deadlines and business expectations?
- Do you have effective consultative arrangements and understand your workers? For example who works for you? What do they do? Do you have contractors as workers? Do you have technical or high risk workers? Do you have workers located overseas?
- Do you know who your health and safety representatives and champions for health and safety are?
- Will another person be acting in your role?
- Will that person have the same responsibility and decision making powers e.g will they be an officer?
- If they are an officer, do they have all the information they need to exercise due diligence?
- If your decision making responsibility is transferred to another officer, do they have all the information to assist them to exercise due diligence?
- Are all relevant managers and supporting workers aware of the change?
So What Does The Information Tell Us About Our Health And Safety?
Measuring health and safety performance provides an insight into management, investment and resourcing decisions. As part of due diligence requirements, officers are required to ensure that the business or undertaking has appropriate processes for receiving and considering information regarding incidents, hazards and risks and responding in a timely way to that information. This can be met by:
- employing a risk management process
- having efficient, timely reporting systems
- empowering workers to cease unsafe work and to request better resources
- establishing processes for considering/responding to information about incidents, hazards and risks in a timely fashion
- measuring against positive performance indicators to identify deficiencies (for example, the percentage of issues actioned within agreed timeframes).
Officers should:
- be accountable for the implementation, verification and review of any change management processes
- ensure health and safety is integrated into business planning and does not get downgraded based on competing priorities, profit margins, and lack of resources
- promote and encourage regular discussion of health and safety at all levels of the business to ensure officers and workers can achieve outcomes based on open communication, consultation, negotiation and agreement
- establish and promote fair and equitable workplace participation and issue resolution processes
- encourage early intervention for incidents and accidents
To assist officers in measuring health and safety performance, they should critically evaluate:
- systems of work
- governance and accountability
- the implementation of policies and procedures
- the measuring of behaviour, and the monitoring of attitudes
- indicators of organisation health—for example, staff surveys, workforce planning, attendance management, etc.
Investing in hazard and incident reporting systems won’t reduce injuries and premiums unless the information is received in a timely manner and properly analysed. Research shows that human factors significantly contribute to 80 to 90 per cent of all incidents. It is therefore important to have a reporting and tracking system that methodically analyses risk with a specific focus on human factors and breaks down general risks into specific risks.
Having clear, effective and workable reporting processes will enable the PCBU to meet its obligations, including notifying the regulator according to the requirements of the WHS laws.
As an officer, you should encourage a reporting culture with clear reporting lines and communication options that does not seek to place blame or punish those who report incidents, near misses and hazards. Establishing an open reporting culture within your organisation will demonstrate to your workers a no blame culture report a near miss, accident or injury or where there has been a failure to adhere to policy or procedure.
You should consider how you as an officer can encourage and support a reporting culture that assists in assessing the risk and hazards to the business as it applies to work health and safety.
Encouraging workers to report near misses and other incidents allows for appropriate and timely remedial or preventive action to be put in place in line with due diligence requirements. You will have a clearer picture of the overall business hazards/risks where effective local reporting procedures are in place that support business policies or procedures and which comply with WHS legislation. Having clear, effective and workable reporting processes will enable the PCBU to meet its obligations.
How Do You Ensure That Compliance Is Being Met?
Part of the due diligence requirements of an officer includes ensuring that processes implemented comply with specific duties and obligations under the WHS Act. These include incident reporting, consultation with workers and ensuring the provision of training and instruction to workers about work health and safety.
This can be met by:
- undertaking a legal compliance audit of policies, procedures and practices
- testing policies, procedures and practices to verify compliance with safety management planning. The PCBU, through its officers should:
- have effective WHS policies, practices, and procedures in place
- document that the PCBU conducts workplace safety audits, identifies hazardous practices and conditions and make the necessary changes to correct these conditions
- provide workers with information to enable them to work safely (in appropriate languages)
- provide the appropriate training and education to workers so that they understand and carry out their work according to the established policies, practices, and procedures
- monitor the workplace and ensure that workers are following the policies, practices and procedures. Written documentation and procedures for progressive disciplining for breaches of safety rules is considered a part of meeting due diligence requirements.
For the purposes of the WHS Act requirements, the duties or obligation of a PCBU do include:
- reporting notifiable incidents
- consulting with workers
- consulting with other PCBUs
- ensuring compliance with notices issued under the WHS Act
- ensuring the provision of training and instruction to workers about work health and safety
- ensuring that health and safety representatives receive their entitlements to training.
Officer Considerations
As an officer, consider:
- how you consult and communicate with your managers, WHS advisers and workers
- the processes and procedures you have in place allow for you to hear and see what is happening at the coal face of your business
- what other methods may be suitable for you to ensure that you are aware of, and involved with, the health and safety aspects of your business—this could be through management committees, WHS committees, regular reporting processes, inspections.
- how you cooperate and coordinate activities with other duty holders • whether you comply with licensing and registration obligations.
Section 27(5)(f)—to verify the provision and use of the resources and processes as they apply to:
(c) ensure that the person conducting the business or undertaking has available for use, and uses, appropriate resources and processes to eliminate or minimise risks to health and safety from work carried out as part of the conduct of the business or undertaking.
(e) to ensure that the person conducting the business or undertaking has, and implements, processes for complying with any duty or obligation of the person conducting the business or undertaking under this Act.
How Do I Know the Systems, Policies and Procedures Are Helping to Protect the Health and Safety of Our Workers?
The scope of your duty as an officer is directly related to the influential nature of your position. Continuous examination and care is required to ensure that the resources and systems of the business or undertaking are adequate to comply with the duty of care required under the WHS Act. This also requires officers to ensure that accountabilities are working effectively. Where you rely on the expertise of a manager or other person, that reliance must be reasonable and relevant independent enquiries and examination should be undertaken by the officer.
It is necessary to measure and evaluate safety performance to enable you to verify the effectiveness of systems, policies and procedures in line with:
- the business structure
- reporting
- technology
- training and information
- auditing
- documentation
- consultation
During the planning stage, procedures for measurement and evaluation of the system should be developed. These procedures should provide information to you, as an officer, on:
- persons responsible for the monitoring and evaluation process
- systems developed for the measurement of WHS performance—for example, a work health and safety information system, which records the number of incidents and accidents, number of hazard inspections and their results per year, etc
- testing methods specific to your agency (for example testing the Emergency Control Organisation via a fire drill, or personal monitoring for employees involved in hazardous operations)
- audit tools to be used, such as WHS-specific audit tools and internally developed audit methods
It is important to evaluate and verify health and safety systems, policies and procedures that are in place are working effectively and to consider opportunities for improvement.
As a leader you should be prepared to learn from safety incidents. Understanding the reasons for the safety incident and taking the necessary steps to address the events leading to the incident will result in improved, safer outcomes for all workers.
The Colombia shuttle explosion could have been avoided if warnings from NASA engineers about a previous foam block incident (failure) on another shuttle booster had been addressed.
The Colombia Accident Board determined—in their 2003 report into the disaster—that management and organisational problems were as much of a factor in the disaster as technical issues. Managers became comfortable with foam strikes on previous missions despite a requirement that debris not strike the shuttle. Concerns of lower level engineers about the strike on Colombia never reached upper management
For this reason, it is necessary to implement a system which will allow corrective action to be taken where required. Corrective action may be necessary to fix a gap in the system as a preventive measure following evaluation. It may also be a reactive measure following an incident in the workplace. It is preferable that any corrective action taken is preventative, and therefore proactive in nature.
Regular reviews of performance and appropriate corrective action will result in a process of continuous improvement. This process should identify:
- reasons why WHS performance may not be meeting organisational targets and objectives (possibly through deficiencies in systems, processes etc.)
- instances of non-compliance with legislative requirements
- opportunities to improve the organisation’s work health and safety performance through adjustments of systems
- changes necessary as a result of the introduction of new technology, plant, equipment, chemicals or work practices
- the effectiveness of any changes made.
Does everything have to be documented?
The WHS Act and Regulations state what records must be kept and the length of time the records must be kept. Keeping other records is optional, however if it is not recorded when it happens, what do you have available to demonstrate you have complied with your due diligence duties in relation to the matter?
Synthesis
The intent of the positive duty placed on officers under the WHS Act is to ensure engagement and leadership by officers in work health and safety management to prevent injury and illness in the workplace. This supports sustainability and improvement in work health and safety performance and workplace productivity.
The way in which activities are undertaken, including the ways in which decisions are reached, consultation and risk assessment are undertaken and so on, are critical in supporting an effective due diligence framework.
The critical elements of exercising due diligence are:
- the things you should know regarding work health and safety matters (section 27(5)(a))
- why the business or undertaking conducts specific operations and the risks and hazards associated with these operations (section 27(5)(b))
- how the business or undertaking applies its resources in complying with the WHS legislation (subsections 27(5)(c) & (e))
- what the information received tells you about the risks and hazards and how the business or undertaking responds (section 27(5)(d))
- verification that the systems, policies and procedures effectively assist in protecting the health and safety of workers (section 27(5)(f)).
These requirements, while not exhaustive, form a basis for you, as an officer, to take action to ensure compliance with work health and safety laws by your organisation.
Taking a whole-of-system thinking approach to exercising due diligence enables the formulation of a plan for accessing information to assist decision making. Combining seemingly unconnected pieces of information that on their own do not necessarily create a need for change, can often provide an insight into wider or more subtle issues that need to be managed before they turn into serious health and safety issues.
Consider the insights, implications, and conclusions arising from working through each of the elements of due diligence.
This examination from a new (informed and considered) perspective casts new light on your former, current, and future knowledge of health and safety in your business or undertaking. Leading questions are a useful device to explore the implications or consequences of the conclusions reached.
What’s Possible, When You Bring All Elements Together— Where to From Here?
This guidance and information aims to assist you, as an officer, to get started and to identify some ways in which you can meet your due diligence obligations.
Aside from the mandatory requirement to exercise due diligence, as an officer in your organisation, you have so much more to gain from taking a proactive approach and making a genuine commitment to the health and safety of all of your workers.
The techniques of effective planning, consultation and communication can spread to other aspects of your organisation, for example:
- worker/management cooperation can increase
- cost of accidents, damage, and lost time goes down
- quality of product, morale, and reputation goes up.
Most importantly, you and the other people in the workplace who share your working life return healthy and safely to your family and friends at the end of the day.

Overview
This fact sheet provides general guidance for persons conducting a business or undertaking (PCBUs) and workers on managing health and safety risks at the workplace. It is based on and should be read together with the Work Health and Safety (WHS) Act and Regulations, the Code of Practice: How to Manage Work Health and Safety Risks and any other applicable codes of practice or guidance material.
Managing Risks to Health and Safety at The Workplace
Managing work health and safety risks involves four steps (see figure below):

- Identifying hazards—finding out what could cause harm
- Assessing risks (if necessary)—understanding the nature of the harm that could be caused by the hazard, how serious the harm could be and the likelihood of it happening
- Controlling risks—implementing the most effective control measure that is reasonably practicable in the circumstances
- Reviewing control measures—ensuring control measures are working as planned.
Control measures must be selected to eliminate the risk, so far as is reasonably practicable. If elimination is not reasonably practicable, the risks must be minimised so far as is reasonably practicable.
PCBUs’ Responsibility for Managing Risk
PCBUs are responsible for managing work health and safety risks. Sometimes several PCBUs may share responsibility with other business operators who are involved in the same activities or who share the same workplace. These PCBUs must consult, cooperate and coordinate activities with all other persons who have a work health or safety duty in relation to the same matter, so far as is reasonably practicable.
Tasks to manage risks may be delegated, but ultimately each relevant PCBU holds this responsibility under the law.
Each PCBU must ensure that relevant workers and their health and safety representatives are involved in the risk management process. PCBUs should also ensure that whoever carries out any step in the risk management process has the necessary skills and experience to do so and understands when specialist help might be needed.
More information and guidance on consultation is available in the Code of Practice: Work Health and Safety Consultation, Cooperation and Coordination.
Consultation and Managing Risks
Consultation with workers and their health and safety representatives is required at each step in managing risks to health and safety at the workplace. By drawing on the experience, knowledge and ideas of workers.
PCBUs are more likely to identify all hazards and choose effective control measures. Workers should be encouraged to report any hazards and health and safety problems immediately so that risks can be managed before an incident occurs.
If there is a health and safety committee for the workplace, it should also be engaged in managing health and safety risks at the workplace.
Using a Consultant
In most cases the relevant PCBU can carry out the risk management steps with the help of workers. External help or advice may be necessary if there is insufficient in-house experience or knowledge, or if risks are complex.
Managing Risks – Who Should Be Covered
Risks must be managed to ensure the health and safety of workers and other people affected by the conduct of the business or undertaking including visitors and customers at a workplace. Special consideration must be given to vulnerable workers including:
- contractors and shift workers who may not be familiar with the workplace, including the systems of work implemented at the workplace
- new and young workers who may be inexperienced or lack the maturity to recognise risks
- workers with poor literacy skills—if staff can’t sufficiently read, write or add, this can affect their ability to understand and follow guidance and instructions and expose them to greater risk
- new or expectant mothers who may be more prone to health-related risks such as physical, biological or chemical risks
- persons with a disability—reasonable modifications to the workplace and work tasks may be required to enable them to work safely.
PCBUs should also think about other people such as members of the public and groups of people who share the workplace (for example childcare centres, nursing homes and sporting venues) when considering how to control risks.
Four Steps to Managing Risks to Health and Safety
-
Identify Hazards—Finding Hazards and Potential Hazards
A hazard is anything that could be harmful to any person. Some hazards will be obvious because they may be common to a particular industry, but others can by more difficult to identify.
Working closely with workers and looking at every task at the workplace will assist in finding potential hazards.
Information and advice about hazards and risks relevant to particular industries and types of work is available from regulators, industry associations, unions, technical specialists and safety consultants.
Manufacturers and suppliers can also provide information about hazards and safety precautions for specific substances (safety data sheets), plant or processes (instruction manuals).
Analyse records of health monitoring, workplace incidents, near misses, worker complaints, sick leave and the results of any inspections and investigations to identify hazards.
If someone has been hurt doing a particular task, then a hazard exists that could hurt someone else. These incidents need to be investigated to find the hazard that caused the injury or illness. Once identified, hazards should be recorded in writing.
-
Assessing the Risks
A risk assessment involves considering what could happen if someone is exposed to a hazard and the likelihood of it happening. A risk assessment can help determine:
- how severe a risk is
- whether any existing control measures are effective
- the action that should be taken to control the risk
- how urgently the action needs to be taken.
A risk assessment does not have to be complex—this will depend on the type of hazards and the information, data and resources that are available. It can be as simple as a discussion with workers or may involve specific risk analysis tools and techniques recommended by safety professionals.
-
Control the Risks – Fixing the Problems
Once the hazards have been identified (and where necessary, any relevant risks assessed) start on the most important step of all—fixing the problems.
The various ways of controlling risks can be ranked from the highest level of protection and reliability to the lowest. This is referred to as the hierarchy of controls.
The most efficient way of controlling risks is to eliminate a hazard, so far as is reasonably practicable. If not reasonably practicable the next step is to minimise the risks so far as is reasonably practicable, by doing one or more of the following:
- Substituting (wholly or partly) the hazard creating the risk with something that creates a lesser risk
- Isolating the hazard from any person exposed to it, and/or
- Implementing engineering controls.
If a risk then remains, the remaining risk must be minimised, so far as is reasonably practicable, by implementing administrative controls. An administrative control means a method of work, a process or a procedure designed to minimise risk, but does not include an engineering control or the use of personal protective equipment (PPE).
Following the implementation of administrative control, if a risk still remains, then the remaining risk must be minimised, so far as is reasonably practicable, by ensuring the provision and use of suitable PPE. A combination of controls should be used if a single control is not sufficient for the purpose.
-
Reviewing Risk Controls
Controlling health and safety risks in the workplace is an ongoing process that needs to take into account changes in the workplace. This is why procedures and risk controls must be reviewed regularly to ensure they are still effective.
Risk control measures implemented to meet work health and safety requirements must be reviewed and as necessary revised to maintain, so far as is reasonably practicable, a work environment that is without risks to health or safety. This includes when:
- the control measure does not control the risk it was implemented to control, so far as is reasonably practicable
- before a change at the workplace that is likely to give rise to a new or different risk to health or safety that the measure may not effectively control
- a new relevant hazard or risk is identified
- the results of consultation required under the laws indicate that a review is necessary
- a health and safety representative requests a review and they reasonably believe that:
- a circumstance referred to above affects or may affect the health and safety of a member of the work group they represent, and
- the control measure has not be adequately reviewed.
When to Assess Risk
A risk assessment is mandatory for certain high risk activities such as entry into confined spaces, diving work and live electrical work.
Although a risk assessment may not be mandatory under the WHS Regulations, it should be conducted when:
- there is uncertainty about how a hazard may result in injury or illness
- the work activity involves a number of different hazards and there is a lack of understanding about how the hazards may interact with each other to produce new or greater risks
- changes at the workplace occur that may impact on the effectiveness of control measures.
A risk assessment is not necessary if:
- laws already require the relevant hazards or risks to be controlled in a specific way—these requirements must be complied with
- a code of practice or other guidance sets out a relevant way of controlling a hazard or risk that is applicable to your situation—this guidance can be followed
- well-known and effective controls that are used in the particular industry, are suited to the relevant circumstances in a particular workplace—these controls may be implemented.
New or different risks associated with a change in work systems or work location should be covered by a specific assessment.
Deciding What Is ‘Reasonably Practicable’
Deciding what is ‘reasonably practicable’ to protect people from harm requires taking into account and weighing up all relevant matters including:
- the likelihood of the hazard or the risk occurring
- the degree of harm that might result from the hazard or the risk
- knowledge about the hazard or risk
- ways of eliminating or minimising the risk, and
- the availability and suitability of ways to eliminate or minimise the risk.
It is only after assessing the extent of the risk and the available ways of eliminating or minimising the risk, that consideration may be given to the cost associated with available ways of eliminating or minimising the risk. A relevant factor at this point is whether the cost is grossly disproportionate to the risk.
Keeping Records
It is good practice to keep records of risk management activities while they remain relevant. Keeping records of the risk management process demonstrates compliance and may help when undertaking subsequent risk assessments.
For most workplace risks there is no set amount of time that records must be kept. However records for certain high risk activities such as entry into confined spaces, diving work and live electrical work must be kept for a prescribed period of time.

This document should be read in conjunction with the Work Health and Safety Act 2011 (WHS Act), Work Health and Safety Regulations 2011 (WHS Regulations) and the Work Health and Safety Code of Practice for Hazardous Manual Tasks (HMT CoP).
-
Identify
What Is a Hazardous Manual Task (HMT)?
A HMT requires a person to lift, lower, pull, carry or otherwise move, hold or restrain any person, animal or thing. HMTs involve one or more of the following characteristics:
Movement
- Repetitive: using the same parts of the body to repeat similar movements over a period of time
Vibration
- Whole body: when vibration is transmitted through the whole body usually via a supporting surface, for example, a seat or floor in heavy vehicles or machinery
- Hand-arm: when vibration is transferred through a vibrating tool, steering wheel or machinery controls.
Posture
- Sustained: where a part of or the whole body is kept in the same position for a prolonged period
- Awkward: where any part of the body is in an uncomfortable or unnatural position; postures that are unbalanced or asymmetrical or that require extreme joint angles, bending, twisting or reaching.
Force
- Repetitive: using force repeatedly over a period of time to move or support an object
- Sustained: occurs when force is applied continuously over a period of time
- High: occurs in any task that a worker describes as physically demanding, a worker needs help to do because of the effort required and/or requires a stronger person or two people to do the task
- Sudden: task where force is applied suddenly and with speed resulting in jerky or unexpected movements while handling an item or load.
Psychosocial Issues
Research states that psychosocial issues can contribute to an increased risk of musculoskeletal disorders.
- Organisational: high workloads, poor leadership and support, low job control, poor change management
- Relationships: Poor relationship with the supervisor, poor relationship with the team, poor reward and recognition.
-
Assess
What Is the Risk of Musculoskeletal Disorders (MSD)s?
The risk of a worker developing a MSD will depend on the following:
- How often and how long specific postures, movements and/or forces are held or performed (repetitive is more than twice per minute and sustained is held for morethan 30 seconds)
- The duration of the task (long duration is more than two hours over a whole shift
- and/or continuously for more than 30 minutes at a time) • If the task involves high or sudden force
- If the task involves vibration
- If there are psychosocial issues involved, such as high workloads
What Are the Sources of Risk?
Consider the following sources of risk:
- Work area design and layout
- The nature, size, weight or number of people, animals or things handled
- Systems of work and organisational issues
- Workplace environment and relationships.
-
Control
When controlling the sources of risk consider the following:
- Is the task necessary?
- Can the source of risk be eliminated or minimised?
- Can mechanical aids be used to perform the task?
- What training is needed to support the control measures?
- Can the job design be amended to reduce identified risk?
Section 17 of the WHS Act, WHS Regulations and HMT CoP require that risks to health and safety be eliminated or minimised so far as is reasonably practicable:
A RISK CONTROL IS HIGHLY RECOMMENDED when:
- repetitive movement or repetitive force is performed more than twice per minute,
- or sustained posture or sustained force is held for more than 30 seconds, and
- the task is performed for more than two hours over a shift or continuously for
- more than 30 minutes at a time
- any high or sudden force is present
- psychosocial issues are identified
- prevention systems are not applied to psychosocial issues
- vibration exists, including whole body and hand-arm vibration.
See www.safeworkaustralia.gov.au for vibration information
-
Review
Continuously monitor and evaluate. Control measures that have been implemented must be reviewed in the following circumstances:
- When the control measure does not minimise the risk so far as is reasonably practicable
- Before a change at the workplace that is likely to give rise to a new or different health and safety risk that the control measure may not effectively control
- If a new hazard or risk is identified
- If the results of consultation indicate that a review is necessary
- If a health and safety representative (HSR) requests a review.

Slips and Trips
Slips and trips result in thousands of injuries every year. The most common ones are musculoskeletal injuries, cuts, bruises, fractures and dislocations but more serious injuries can also occur.
Slips occur when a person’s foot loses traction with the ground surface due to wearing inappropriate footwear or when walking on slippery floor surfaces such as those that are highly polished, wet or greasy.
Trips occur when a person unexpectedly catches their foot on an object or surface. In most cases people trip on low obstacles that are not easily noticed such as uneven edges in flooring, loose mats, opened drawers, untidy tools or cables from electrical equipment. Falls can result from a slip or trip but many also occur during falls from low heights such as steps, stairs and curbs, falling into a hole or a ditch or into a body of water.
The Role of PCBUs
PCBUs must manage the health and safety risks associated with slips and trips by eliminating the risk so far as is reasonably practicable, and if that is not reasonably practicable, minimising the risk so far as is reasonably practicable. This involves a systematic approach to:
- identify hazards
- if necessary, assess the risks associated with these hazards
- implement and maintain risk control measures
- review risk control measures.
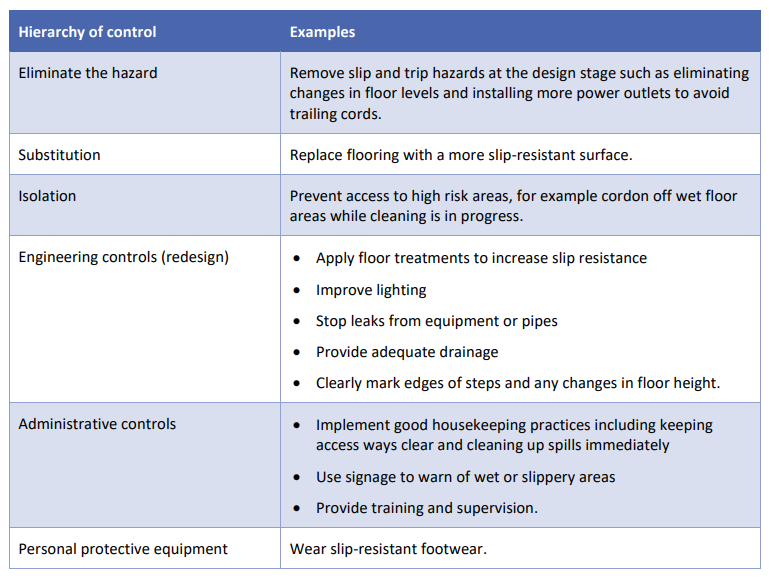
There are various ways to control the risk of slips and trips, listed below in order of their effectiveness (known as the hierarchy of controls [see table below]).
More than one control measure may be needed to provide the best protection. [A checklist to assist with the identification of slip and trip hazards and the selection of appropriate control measures is at the end of this fact sheet].
Identifying Slip and Trip Hazards
Common slip hazards include:
- spills of liquid or solid material
- wet cleaning methods
- wind-driven rain or snow through doorways
- a sudden change in floor surface, for example joins between carpet and polished timber
- change from wet to dry surface
- dusty and sandy surfaces
- the incline of a ramp
- loose or bumpy flooring
- low light levels
- use of unsuitable footwear.
Common trip hazards include:
- ridges in floors or carpets
- worn floor coverings or broken tiles
- potholes and cracks in floors
- changes in floor level
- thresholds and doorstops
- floor sockets and phone jacks
- cables from power extension units
- loads that obstruct vision
- obstacles in traffic areas.
Selecting Control Measures – Design of Facilities
The best way to eliminate slips and trips is to build and design facilities with safety in mind. The following are some general matters which should be considered during the design stage.
For Floor Design:
- Minimise any changes in the floor level. If levels must change, use ramps rather than steps when connecting pedestrian pathways.
- Ensure the maximum ramp slope does not exceed 1:12.
- Use slip-resistant floor tiles.
- Avoid sudden transitions in floor surface texture if possible. If such transitions occur, ensure good lighting and visual cues highlight the change.
For The Design of Stairs:
- All risers and treads should be uniform throughout a flight of stairs.
- Variations in the riser and tread should be reasonable—the riser ranges from 150 – 175mm and the tread ranges from 225 – 320mm, trips can easily occur for risers less than 75mm.
- The elevation of any flight of stairs should be designed between 15° and 55°.
- A landing should be introduced every 16 steps in a flight of stairs.
- Consider whether handrails are required, including if it is not reasonably practicable to implement the above controls.
For Lighting Design:
- Ensure both internal and external stairways are well lit.
- Areas such as corridors, walkways, staircases and lifts, should have an illuminance of at least 100 lux, so far as is reasonably practicable.
For The Design of Drainage:
- Provide means of containing and draining fluids at machines or processes.
- Provide drains as close as possible to any source of water or liquid that is frequently generated.
- Use floor grates where work tasks generate a lot of water or liquid.
- Ensure grates in walkways or aisles are slip resistant.
When Designing Storage:
- Provide ample storage space to avoid materials being placed in aisles.
- Ensure procedures for the return of tools to designated areas are in place.
When Designing Work Procedures:
- Develop procedures that avoid the build-up of rubbish throughout a production process, for example using pre-cast units instead of formwork and bar-bending construction methods in construction work.
- Choose or replace machinery that frequently generates noise, dust, fumes or smoke.
Selecting Control Measures – Housekeeping
Good housekeeping helps prevent slips and trips. Examples of control measures include:
- training staff to recognise slip and trip hazards and the importance of good housekeeping
- setting up standards and procedures for storage and cleaning
- checking and storing usable inventories, discarding any unwanted items • implementing safe systems of work and any relevant signage for timely and efficient reporting and clean up of spills
- providing sufficient rubbish or recycling bins
- using appropriate containers for rubbish if it is likely to contain sharp objects
- developing a cleaning schedule that assigns workers to take charge of cleaning workplaces, and
- encouraging workers to clean their workplaces daily before they leave, so far as is reasonably practicable.
Selecting Control Measures – Safety Training
All workers share responsibility for housekeeping and cleanliness at the workplace. Work health and safety training not only assists workers to become more aware of slip and trip hazards and the relevant control measures, but also helps to prevent injuries.
Training should include:
- awareness of slip and trip hazards
- identifying effective control measures
- duties of workers. Selecting control measures—personal protective equipment Personal protection equipment (PPE) including slip resistant footwear should only be used:
- when there are no other practical control measures available (as a last resort)
- as an interim measure until a more effective way of controlling the risk can be used
- to supplement higher level control measures (as a backup).
When selecting and purchasing footwear consider whether it has good slip resistance properties, in addition to any other required safety features. For example:
- in wet conditions—the shoe sole tread pattern should be deep enough to help penetrate the surface water and make direct contact with the floor
- in dry conditions—the shoe sole tread pattern should be flat bottom construction which grips the floor with maximum contact area, and
- urethane and rubber soles are more effective than vinyl and leather soles for slip resistance. Sole materials that exhibit tiny cell like features will provide the added benefit of slip resistance.
Controlling The Risks of Slipping
Floor treatments that improve slip resistance are those which increase the surface roughness of the flooring. The main floor treatments are sand blasting or grinding, chemical etching, coating with resins, and using floor mats or adhesive anti-slip strips.
Examples of different floor types are:
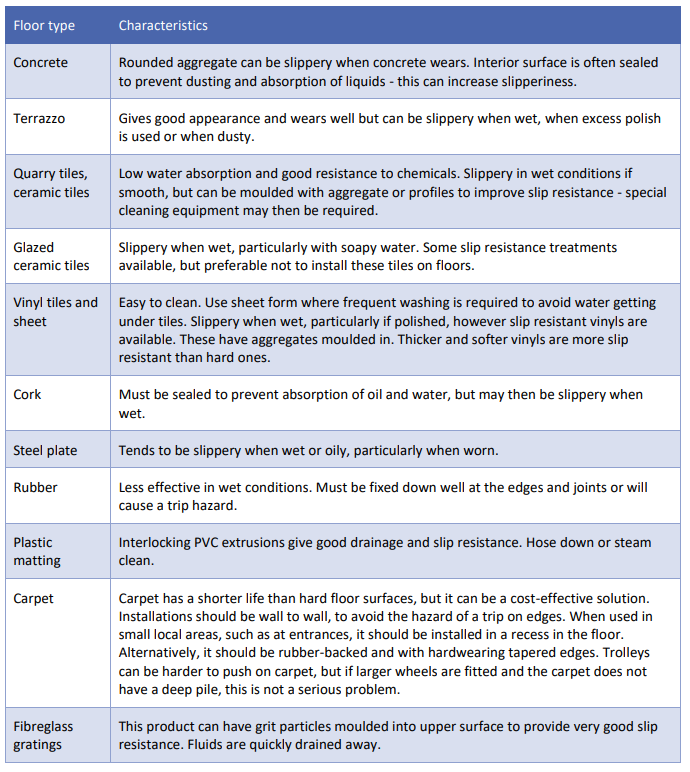
Ways to eliminate or minimise slipping hazards due to liquid and waste from machinery include:
- modify the machinery to prevent leakage
- install exhaust systems to remove dusts or that would otherwise settle on floors
- use a tray to collect liquid and waste.
Ways to eliminate or minimise slipping hazards due to rainy days include:
- have absorbent flooring materials at entrances
- provide facilities for leaving umbrellas at entrances
- provide easy access to equipment and materials for cleaning up water on the floor.
Ways to eliminate or minimise slipping hazards due to accidental spills include:
- clean up water or oily spills immediately – use absorbent paper or powder for cleaning up any oily residues
- thoroughly dry floors after cleaning
- erect warning signs at areas with a high risk of spills.
Controlling The Risks of Tripping
Ways to eliminating tripping hazards include:
- provide storage areas separate to work areas
- provide sufficient storage systems to keep materials out of aisles
- provide sufficient power sockets and computer service jacks to minimise or remove the requirement for cords on the floor (where possible)
- remove or cover protruding sockets on the floor
- securely stack goods and avoiding single towering stacks
- hang power cords over work areas rather than on the floor
- clean up workplaces and remove rubbish or obstructions regularly
- display visual cues, such as warning strips and signs to alert pedestrians about changed or uneven surfaces.
Shared Workplaces
In shared workplaces PCBUs must consult, cooperate and coordinate activities with all other persons who have a work health or safety duty in relation to the same matter, so far as is reasonably practicable.
In shared workplaces PCBUs may have varying degrees of control over the physical workplace, for example, flooring, lighting and cleaning. They must do what is reasonably practicable in the circumstances to prevent slips and trips at the workplace. They can do so by consulting each other and working together to implement appropriate control measures.
For example:
- At a shopping centre, the centre management is responsible for ensuring common access floor surfaces are well maintained and kept free of obstructions.
- Where shop owners need to move stock in and out of stores or if they wish to display goods outside of the store, they must consult, cooperate and coordinate with the centre management to avoid injuries from occurring.
- Where spills have occurred in the main access areas, the centre management must make arrangements to ensure the spill is cleaned up in a timely way.
Further guidance is available in the Code of Practice: Work Health and Safety Consultation, Cooperation and Coordination.
More Information
More work health and safety resources are available on the Safe Work Australia website.
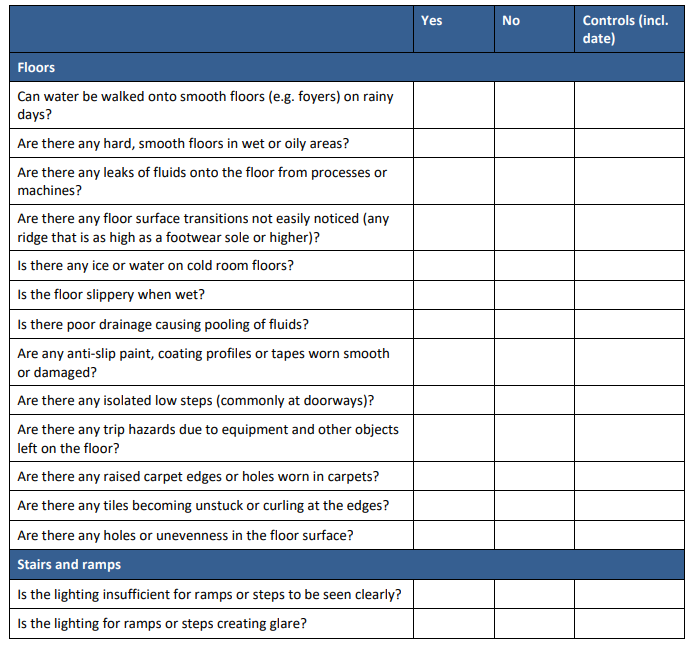
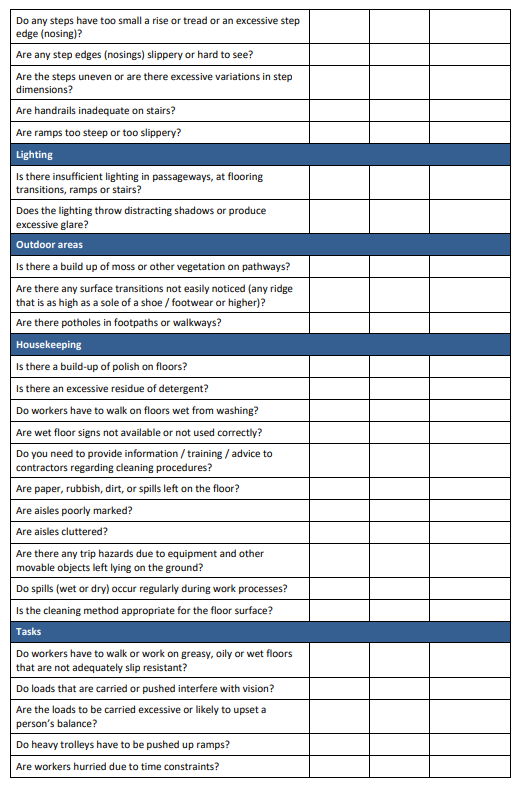
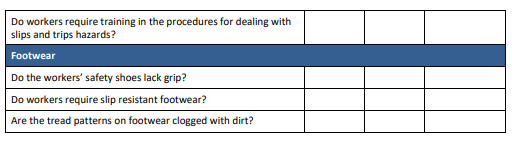
Checklist – Preventing Slips and Trips at Work
This checklist may be used to identify hazards and control slips and trips in the workplace. It is not an exhaustive list of all the items you may need to consider. You should keep a copy of your records.
If you answer “yes” to any of the questions below you must ensure controls are implemented to eliminate or minimise the risk of slips and trips.

Overview of Work-Related Stress
Stress is a term that is widely used in everyday life and most people have some idea of its meaning. Work-related stress is recognised globally as a major challenge to workers’ health, and the health of an organisation.
Work-related stress describes the physical, mental and emotional reactions of workers who perceive that their work demands exceed their abilities and/or their resources (such as time, help/support) to do the work. It occurs when they perceive they are not coping in situations where it is important to them that they cope.
A worker’s response to stressors at work may be positive or negative for worker wellbeing, depending on a number of factors. In the vast majority of instances, people adjust to stressors and are able to continue to perform their normal work duties. While stress itself is not a disease, if it becomes excessive and long-lasting it can lead to mental and physical ill-health
Your Legal Obligations
Work-related stress leading to illness, injury and weakened organisational performance can come from many sources, both work and non-work. Employers are not able to control workers’ personal lives and the stressors they may encounter there, however they do have a legal obligation to minimise their exposure to work-related factors that can increase the risk of work-related stress.
The Work Health and Safety Act 2011 imposes a legal duty on business operators to do what is reasonably practicable to eliminate or minimise risk to worker health and safety. This duty extends to protecting workers from the risk of harm from stressors at work.
Risk Factors for Work-Related Stress
The key to reducing the effects of work-related stress is to understand what organisational, environmental and individual characteristics may lead to stress in the first place.
Organisational
It is important to understand the types of organisational stressors people can be exposed to when examining work-related stress. A simplified model is shown in Figure 1 (below). The model identifies the kinds of organisational stressors or risk factors that might lead to workers experiencing stress and sustaining psychological and/or physical ill-health.

Environmental
Environmental stressors such as physical, chemical or biological agents can influence the worker’s comfort and performance in his or her work environment, and might contribute to a stress response. These factors can cause stress on their own, but often act to exacerbate a person’s response to another stressor.
Types of environmental stressors include:
- noise
- temperature and humidity
- lighting
- vibration
- air quality
- unguarded plant and equipment.
Individual
People respond to stressors at work in different ways. It has been suggested that this can, in part, be related to physiological and/or personality factors (e.g. resilience). Worker well-being appears to benefit from a combination of challenging work, a supportive atmosphere and adequate resources. While it is important to recognise these individual differences and to match jobs and tasks to individual abilities, this does not reduce an employers legal duty to minimise workers’ exposure to risk factors for work-related stress and to ensure the workplace does not exacerbate an existing illness.
Outcomes of Exposure to Work-Related Stress
Possible Health Effects
Short-lived or infrequent exposure to low-level stressors are not likely to lead to harm, in fact short-term exposure can result in improved performance. When stressful situations go unresolved, however, the body is kept in a constant state of stimulation, which can result in physiological and/or psychological changes and illness.For example:
Physical: headaches, indigestion, tiredness, slow reactions, shortness of breath
Mental: difficulty in decision-making, forgetfulness
Emotional: irritability, excess worrying, feeling of worthlessness, anxiety, defensiveness, anger, mood swings
Behavioural: diminished performance, withdrawal behaviours, impulsive behaviour, increase in alcohol and nicotine consumption
Common longer-term health issues linked to stress include cardiovascular disease (CVD), immune deficiency disorders, gastrointestinal disorders, psychiatric/psychological illness (PPI) and musculoskeletal disorders.
Possible Effects on Organisational Performance
Increased stress levels of workers in an organisation can lead to diminished organisational performance as measured by the following:
- productivity and efficiency may be reduced
- job satisfaction, morale and cohesion may decline
- absenteeism and sickness absence may increase
- there may be an increase in staff turnover
- accidents and injuries may increase
- conflict may increase and the quality of relationships may decline
- client satisfaction may be reduced
- there may be increased health care expenditure and workers’ compensation claims.
The effects of work-related stress on organisational performance provide good reasons — above and beyond legal duties and the direct financial and human costs — as to why employers and other duty holders should reduce workers’ exposure to workplace stressors.
A Risk Management Approach to Work Related Stress
Risk management is a four-step process for controlling exposure to health and safety risks associated with hazards in the workplace. The Work Health and Safety Act 2011 asserts that, to properly manage exposure to risks, a person must:
- identify hazards
- . assess risks if necessary
- control risks
- review control measures to ensure they are working as planned.
Many of the discussions about stress risk management have traditionally been focussed on individuals within an organisation who are already distressed. This approach is not only costly, but it also means that the employer or business operator may not be fully meeting their duty to eliminate or minimise risks to worker health and safety from being exposed to stressors at work.
The risk of work-related stress may be present in any workplace. Employers should apply the risk management process (illustrated in Figure 1) to eliminate or minimise, as far as reasonably practicable, exposure to potential causes of work-related stress.
Step 1: Identify The Hazards
The first step in the risk management process is to identify workplace hazards. This means looking for those things in the workplace that have the potential to cause harm. The source of work-related stress can be determined by evaluating: productivity levels, rates of absenteeism, separation rates/turnover, exit interviews, staff engagement/ morale, customer feedback, peak/seasonal demands, analysing incident reports and data trends.
Step 2: Assess and Prioritise the Risk
This step involves assessing the likelihood and consequences of injury or illness that may result from exposure to workrelated stressors. Stressors or risk factors for work-related stress include:
- work demands (emotional, mental, physical)
- low control
- poor support
- lack of role clarity
- poorly managed change
- poorly managed relationships
- low levels of recognition and reward
- organisational injustice.
How to Conduct a Risk Assessment
Risk factors for work-related stress can be assessed by understanding worker complaints, observing interactions between workers, gaining feedback from workers, having one-on-one discussions with workers and through the use of focus groups or a worker survey.
Focus groups are small groups (typically 6-10 people) from across the organisation. The purpose of a focus group is to provide a forum for assessing the risk of exposure to work-related stressors. This is done by considering each of the stress risk factors listed above and how they may or may not apply to their workplace. Another effective approach to finding out about work-related stressors is to administer a worker survey. Surveys can be an important tool in soliciting which stressors are present in the workplace, evaluating the degree to which they are affecting workers and pinpointing where they are originating. When undertaking a worker survey, one must consider the size of the group to be surveyed, how participants are to be selected and how survey results will be fed back to staff. Anonymity must be guaranteed throughout the entire process.
Findings from focus groups or worker surveys would then inform a decision about the likelihood and consequences of injury or illness from exposure to work-related stress and make it clear which risk factors are contributing to that risk.
Step 3: Control Risks
After assessing the risk and determining which factor(s) have the greatest contribution to that risk, the most appropriate control measure(s) that are reasonably practical in the circumstances need to be selected and implemented. When selecting a particular control, it is important to be able to justify why it was chosen over a different measure. For work-related stress, deciding on control measures usually means altering a problem risk factor. For instance, reducing work demands, increasing the level of control a worker has over his or her job, and increasing the amount of peer and/or supervisor support a person is receiving.
Examples of control measures to manage the risk of work-related stress include:
- improving supervisor/managerial skills through coaching, mentoring and/or training
- planning workloads to meet potential demands
- setting clear performance goals/accountability
- ensuring role clarity and reassessing job descriptions
- setting new or adjusting current HR procedures
- providing assistance (e.g. an employee assistance program)
- communicating policy and availability of assistance
- checking understanding and implementation of changes
- promoting effective early rehabilitation
Step 4: Review Control Measures
The last step of the risk management process is to review the effectiveness of the control measures that have been implemented to ensure they are working as planned. When reviewing the effectiveness of control measures, it is important to weigh up whether the chosen controls are effective or whether they need some modification.
Risk management for work-related stress is not a one-off exercise, but something that must go on continually in the organisation. The dynamics and complexity of organisations can mean that changes such as a new supervisor, new workers or new processes or procedures can have marked, unexpected and unplanned effects on the stress levels of workers.

Anxiety, Stress and Burnout in the Human Services
It is not be surprising that social welfare work has been found to be especially anxiety provoking due to the macro context of the human services, its focus on human beings, their complex problems and relationships, and emotionally-charged situations (Coholic and Blackford, 1999; Jones et al., 1991; Strozier and Evans, 1998). However, the empirical research is not consistent in this regard as some comparative studies have found similar levels of anxiety in other occupations. Social workers’ anxiety has been found to be positively associated with depression (Jones et al., 1991) and burnout (Jayaratne et al., 1986), and is moderated by supervisors’ emotional and other supports (Koeske and Koeske, 1989). However, conceptualising the differences between anxiety and stress has been problematic, and most studies have focussed on the ‘burnout’ concept, often using it interchangeably with occupational stress, work stress, distress and vicarious trauma (Adams et al., 2001; Dollard et al., 2001; Strozier and Evans, 1998).
‘Work stress’ has been defined as a “condition or intermediate arousal state between objective stressors and strain”, with strain being “reactions to the conditions of stress” (Dollard et al., 2001, p.15). On the other hand, the concept of ‘burnout’ describes the longer-term process where chronic stressors lead to occupational stress experienced by those in people-oriented professions that results in them being unable to cope with their work psychologically and emotionally (Barak et al., 2001; Maslach, 1976). It has been conceptualised as involving the three components of:
- Emotional exhaustion;
- Depersonalisation of clients; and
- Decreased personal accomplishment (Maslach, 1998).
Emotional exhaustion is characterised by feeling emotionally overextended and depleted, while depersonalisation entails a practitioner becoming overly cynical and detached to others, particularly clients, and diminished personal accomplishment is evidenced when workers demonstrate reduced self-efficacy and productivity (Maslach, 1998). Emotional exhaustion is the burnout component that is closest to occupational stress (Koeske and Koeske, 1989, 1993). However, most research of burnout has involved human service workers, inviting the criticism that it is a flawed concept (Demerouti et al., 2001; Jones et al., 1991; Soderfeldt et al., 1995) that merely re-labels emotional exhaustion (Wallace and Brinkerhoff, 1991) and reflects the predominance of “feeling type” people in the human services (Garden, 1989).
Nevertheless, some authors (Maslach, 1998; Powell, 1994) argue that maintaining the three dimensions of burnout is critical because this ensures that burnout is an interpersonal framework rather than a narrow concept of stress reactions to work or other stressors. However, a re-examination of the dimensions of burnout found evidence linking work stress only with emotional exhaustion (Wallace and Brinkerhoff, 1991) and this is supported by other researchers (Koeske and Koeske, 1989, 1993; Koeske and Kirk, 1995a) who noted that detachment, a dimension of the depersonalisation aspect of burnout, is also an effective tool against it, as detached concern can assist a worker to prevent emotional overload.
Social work practitioners have generally been found to experience higher stress and lower well-being levels than other occupations (Bennett et al., 1993; Bradley and Sutherland, 1995; Collings and Murray, 1996; McLean and Andrew, 2000; Strozier and Evans, 1998; Um and Harrison, 1998), particularly statutory workers (Balloch et al., 1998; Dollard et al., 2001). In addition, there is evidence of social workers having higher levels of depression than others (Gibson et al., 1989) although the results are inconsistent (Jones et al., 1991).
On the other hand, some studies have found that social workers and human service practitioners have lower levels of stress than others (Demerouti et al., 2001; Soderfeldt et al., 1995). It has also been argued that the reported levels of stress, anxiety and burnout experienced by human service practitioners are relatively low, especially when viewed alongside the generally high levels of job satisfaction (Pottage and Huxley, 1996; Poulin, 1994; Powell, 1994). As Marriott et al., (1994, p.204) note, “One could speculate that social workers complain about or downgrade various aspects of their jobs but are nevertheless reasonably content.”
Vicarious Trauma
Over the past decade the concept of ‘vicarious trauma’ has been increasingly studied because of its perceived adverse consequences for professionals working with traumatised victims, although its prevalence remains unclear. Vicarious trauma has been defined as “the enduring psychological consequences for therapists of exposure to traumatic experiences of victim clients” (Schauben and Frazier, 1995, p.53), although it is arguable that it is an equally valid phenomenon for all human service workers who are exposed in a secondary fashion to client trauma.
Its symptoms may include a decreased emotional and physical energy, bystander guilt, anxiety, depression and PTSD, disconnection from loved ones, social withdrawal, and increased sensitivity to violence (Dane, 2000; Sexton, 1999). Physical signs of stress can also accompany these symptoms. Other signs include disruption to self-protective and safety beliefs, changed worldviews, helplessness, cynicism and despair (Cunningham, 1999; Sexton, 1999). There is said to be a generally faster recovery from these symptoms than from burnout (Sexton, 1999). Although it remains a nebulous concept and has been used interchangeably with terms such as countertransference, secondary traumatisation, burnout, and compassion fatigue (Dane, 2000; Illiffe and Steed, 2000; Sexton, 1999), there is some empirical evidence to suggest that it is conceptually different from burnout (Schauben and Frazier, 1995).
In either event, it is a normal reaction to empathic engagement with clients who have suffered significant and traumatic events and results from an accumulation of exposure experiences (Sexton, 1999). It goes, so to speak, with the territory of trauma counselling and possibly with many other human service worker roles and functions. Whilst there has not been a lot of research of vicarious trauma, it has been found among domestic violence workers (Coholic and Blackford, 1999; Illiffe and Steed, 2000), trauma therapists (Perlman and Mac Ian, 1995) and sexual assault counsellors (Schauben and Frazier, 1995). Higher levels have been found to be associated with burnout (Adams et al., 2001) and higher caseloads of traumatised clients (Schauben and Frazier, 1995), but not with a prior history of trauma or assault for the worker (Adams et al., 2001; Schauben and Frazier, 1995).
Sources of Stress in The Human Services
The overwhelming conclusion of the research is that structural work stressors, rather than personal characteristics, are the most influential factors affecting the incidence and intensity of burnout (Barak et al., 2001; Bennett et al., 1993; Dollard et al., 2001; Zastrow, 1999), although there are contradictory findings about which factors are involved. Furthermore, it has been found that burnout can be moderated by organisational, professional and personal social support (Um and Harrison, 1998; Zunz, 1998). Interestingly, whilst client experiences are theoretically identified as contributing factors in the process of burnout, investigations have usually failed to establish a link (Barak et al., 2001; Dollard et al., 1999).
Work Factors
There are numerous work-related factors identified in the literature as contributing to work stress and burnout, and these can be placed into the following general groups: particular practice fields, work role issues, organisational structure and culture, high workloads, low levels of control and autonomy, supervision practices, lack of accomplishment and efficacy, violence and conflict, and racism within the organisation. However, there is increasing evidence that a combination of high job demands and low supports is the critical factor in burnout (Dollard et al., 2001).
Studies of burnout and work stress have been conducted across various positions, occupations and practice fields in the human services such as child welfare and protection, mental health, hospitals and community health, disability, generic social services, and support services for the military. Very few studies have addressed the issue of burnout and work stress in non-government, not-forprofit and for-profit agencies. There have been a number of findings indicating that child welfare and child protection work are associated with higher levels of burnout and perceived stress (Gold, 1998; Jayaratne et al., 1986; Jones et al., 1991; Le Croy and Rank, 1987; Samantrai, 1992; Thorpe et al., 2001). It is suggested that the contested and conflictual nature of this sort of statutory work leads to elevated stress for the workers involved who often tread a difficult path in being accountable, balancing the interests of all parties, and ensuring children are protected from abuse.
Social workers have also been found to have higher burnout and stress levels than other human service workers (Bennett et al., 1993; Dollard et al., 2001; McLean and Andrew, 2000) and this has been suggested as resulting from their statutory roles, somewhat limited autonomy and the complex decisions they are often required to make. Role ambiguity and role conflict for social workers and human service workers have consistently been found to be positively associated with levels of emotional exhaustion, burnout and work stress (Balloch et al., 1998; Barak et al., 2001; Dollard et al., 2001; Siefert et al., 1991). However, Um and Harrison (1998) recently used LISREL linear structural relation techniques to examine the process of stress-strain (burnout)-outcome (job satisfaction) in 166 Florida social workers, and concluded that role conflict, but not role ambiguity, intensified burnout and job dissatisfaction.
The organisational structure, culture and climate have also been found in some studies to contribute to higher levels of burnout and stress (Sundet and Cowger, 1990). For example, Bradley and Sutherland (1995) used a quantitative and qualitative research design to compare a group of British social workers and home help workers. The social workers reported stress resulting from the organisational structure and climate including factors such as inadequate resources, time pressures, paper work and lack of performance feedback. Dollard et al., (2001) also found organisational processes such as unfair job selections were related to perceptions of work stress. Poor employer-employee relations have also been identified as problematic (McLean and Andrew, 2000). Perhaps more important is the organisational culture with respect to work stress. Thompson et al., (1996) found in a comparative study of three British local authority social service departments that work groups could develop and embrace a ‘culture of stress’ that reflects and contributes to higher levels of stress. They concluded that management had a critical part to play in creating the vision and circumstances to prevent this.
The relationship between large caseloads and stress, although intuitively linked, has not been consistently born out by the empirical evidence, perhaps due to measurement difficulties (See Egan and Kadushin, 1993; Koeske and Koeske, 1989). For example, LeCroy and Rank (1987) found no significant relationship between social workers’ job performance variables such as the amount of overtime, direct client contact, practice experience and burnout, but Barak et al., (2001) identified it as a significant factor in their review of 25 studies of the antecedents to turnover in human service practitioners. There is, however, stronger evidence regarding the negative impact of overall workloads on work stress (Bradley and Sutherland, 1995; Collings and Murray, 1996; Sundet and Cowger, 1990). Furthermore, when practitioners have limited control and autonomy over their work, burnout and stress levels tend to be higher and job satisfaction lower (Barak et al., 2001; Balloch et al., 1998; Guterman and Jayaratne, 1994; Koeske and Kirk 1995b; McLean and Andrew, 2000; Poulin 1994, 1995). However, high workloads appear to be particularly problematic when they translate to high job demands that are combined with low control and autonomy by the worker, and low resources and support (Demerouti et al., 2001; Dollard et al., 2001; Maslach, 1998; Soderfeldt et al., 1995). This combination has been demonstrated to be associated with significant negative outcomes for the individuals and organisations concerned.
The importance of effective and supportive supervision has been consistently identified as of pivotal importance with respect to job satisfaction and moderating the effects of work stress while poor supervision has been found to contribute to higher work stress (Dollard et al., 1999, 2000; Wilcoxon, 1989; Winefield et al., 2000). Dissatisfaction with supervision has been found to be associated with higher levels of stress and may be a potent source of it, and trigger a decision to leave (Collings and Murray, 1996; Samantrai, 1992). Furthermore, the quality of supervision has been found to be an important element in both supporting workers and controlling the demands placed on them (Jones et al., 1991). For example, Grasso (1994) undertook a two-year study of management styles and found that supportive and participatory supervision of staff was related to higher job satisfaction. However, collegial support may be even more important than supervisor support as a moderator of burnout (Dollard et al., 2001; Himle et al., 1989a, 1989b; Um and Harrison, 1998).
Some writers have claimed that the strongest factor causing burnout for clinical workers is lack of therapeutic success (Ratliff, 1988), but others have found it not to be a factor (Himle and Jayaratne, 1990; Wallace and Brinkerhoff, 1991). However, most studies have identified that practitioners’ self efficacy is inversely related to levels of burnout and job dissatisfaction, although its precise contribution as a preventative measure, moderating factor or consequence of burnout remains unclear (Barak et al., 2001; Dollard et al., 2001; Koeske and Koeske, 1989, 1993; Zunz, 1998).
There has been increasing attention given to the influence of violence and conflict in the workplace and its effects on work stress, especially when associated with a lack of recognition and support (Smith and Nursten, 1998). This issue has been particularly important in statutory services in Great Britain. For example, Balloch et al., (1998) conducted a longitudinal study using quantitative and qualitative methodologies and found a strong association between violence, threats of violence and verbal abuse, and stress levels. They concluded that rising stress levels may well be associated with dealing with increasing levels of workplace violence.
The issue has also been recently identified as contributing to work place stress in a large-scale study of a statutory child welfare and juvenile justice agency in Australia (Dollard et al., 2001). The issue of racism and its effects on occupational stress in human service agencies has also been given increasing attention, although the evidence is mixed. A British study (Collings and Murray, 1996) found no relationship while a U. S. study found that perceptions of cultural sophistication within the organisation were associated with occupational stress levels for Latino social workers (Gant and Guitierrez, 1996).
Non-Work Factors
As noted earlier, the research findings indicate that personal and demographic characteristics play a limited role in the work stress and burnout process, with these factors mostly acting as moderating influences rather than causal factors or sources of stress (Gutek et al., 1988; Jayaratne et al., 1983). There are equivocal findings with respect to the influence of age on work stress with Collings and Murray (1996) finding that older workers tended to have higher levels, whereas Barak et al., (2001) found the opposite in a review of burnout and turnover research. Most studies have not found gender to be an influential factor (Barak et al., 2001; Dollard et al., 2001; Collings and Murray, 1996). However, there is evidence to suggest that a practitioner’s pre-existing level of psychological well-being is negatively related to subsequent levels of emotional exhaustion and job dissatisfaction (Koeske and Kirk, 1995a). Zunz (1998) examined the influence of resiliency on burnout and found that those workers who were more resilient and also received social support tended to experience lower levels of burnout. With respect to other personal characteristics, Dollard et al., (2001) found that ‘trait anxiety’ and ‘financial worries’ had a significant positive relationship with psychological strain.
Practitioners with a high degree of personal commitment to their profession and work have been found to be more likely than others to have greater control of their work, experience less stress, and have higher job satisfaction (McLean and Andrew, 2000), and to also be more likely to stay with their employer (Barak et al., 2001; Rycraft, 1994). Commitment may well be an important personal and professional value base in practitioners’ perceptions of work stress.
Spousal support has also been found to be negatively associated with burnout (Barak et al., 2001; Davis-Sachs et al., 1985; Jayaratne et al., 1986), and positively related to job satisfaction in human service workers (Dollard et al., 2001). However, whilst home-work conflict, such as work intruding on family life, has been found to be associated with psychological strain for human service workers (Dollard et al., 2001), Barak et al., (2001) found that it was not central to turnover considerations. The lack of influential non-work factors identified in the many studies of burnout and turnover in the human services has been consistent over the two decades of research and reinforces the primacy of organisational responses to address these issues.
Consequences of Work Stress in The Human Services
Organisational Outcomes
Despite the conceptual and methodological problems in stress research, there is strong empirical evidence associating work stress with adverse organisational outcomes that are costly in human resource and financial terms (Barak et al., 2001). The direct costs of turnover such as expenses incurred during recruitment, training and separations, are compounded by the indirect costs such as the reduced efficiency of co-workers and new staff, as well as the potential loss of trust and confidence by agency clients unhappy with changed services and staff (Barak et al., 2001). However, quantifications of the extent of the overall costs to individual organisations or the sector as a whole are difficult to obtain, frequently because public disclosure may be embarrassing and counterproductive to recruitment strategies or the public profile of agencies.
In many senses, the burnout-job satisfaction-turnover problems are circular in nature because organisational factors and high workloads increase work stress, which contributes to staff turnover that places greater burdens on the staff who remain, who in turn become more stressed and dissatisfied, and more likely to consider moving on etc. Alternatively, unhappy workers may stay on and thereby create a cumulative agency problem (Koeske and Kirk, 1995a). Unhappy and stressed workers who feel trapped in their agency may contribute to the mythology and overstatement of the burnout problems that occur, as well as the understatement of the career benefits of human service practice. Nevertheless, the occupational stress issues are substantial and lead to many organisational difficulties, and cause considerable personal distress to those affected. Work stress and strain in the human services have been found to be associated with a range of adverse factors and outcomes including decreased job satisfaction and work performance (Barak et al., 2001; Cooper et al., 1988; Gutek et al., 1988; McLean and Andrew, 2000) and increased absenteeism (Kirk et al., 1993; Koeske and Koeske, 1989; Lyons et al., 1995; Ramanathan, 1992). Higher staff turnover (Barak et al., 2001; Lonne, 2001) and elevated rates of intention to quit have also been identified as adverse consequences (Barak et al., 2001; Ramanathan, 1992; Koeske and Kirk, 1995b), although the relationship between intention to quit and actually leaving is not a linear one (Kirk et al., 1993; Koeske and Kirk, 1995a).
However, there is a paucity of evidence with respect to demonstrating and quantifying the extent to which the work performance of those who experience burnout is adversely affected. We remain unsure about exactly how stressed practitioners respond to their situations and the ways in which this affects their work within the organisational and community contexts, and with client outcomes. These all remain critical issues that demand further research.
Personal Outcomes
The adverse outcomes for social workers and human service practitioners from work stress and burnout can be profound and debilitating, elevating it to a major occupational health and safety issue (Dollard et al., 2001). Those affected are vulnerable to a number of adverse consequences for their physical and psychological well-being (Koeske and Kirk, 1995a). There is empirical evidence associating high work stress for practitioners with poorer health outcomes as measured on the GHQ (Balloch et al., 1998; Dollard et al., 2001; McLean and Andrew, 2000). Furthermore, a range of somatic symptoms and stress-related complaints has been linked to work stress including insomnia, exhaustion; stomach problems, dietary complaints, high blood pressure etc (Adams et al., 2001; Bradley and Sutherland, 1995; Gold, 1998). For some, this leads to increased alcohol and drug intake (Fewell et al., 1993; Strozier and Evans, 1998).
Moreover, elevated rates of psychological distress such as anxiety and depression have also been associated with work stress, especially when the practitioner receives lower social support (Bennett et al., 1993; Gibson et al., 1989; Jones et al., 1991). Increased levels of cynicism and negativity have also been identified as a consequence of work stress (Corcoran, 1987; Kirk et al., 1993; Maslach, 1998), along with depersonalisation of clients (Koeske and Koeske, 1993) and feeling alienated (Powell, 1994). Apart from these serious complaints, high stress and burnout has been found to be a significant factor leading to job dissatisfaction and turnover (Barak et al., 2001; Maslach, 1998; Um and Harrison, 1998).
A number of adverse personal outcomes are cited in the literature with respect to vicarious trauma. Besides burnout-like symptoms of exhaustion, irritability and somatic complaints, there is evidence that practitioners may experience anxiety and depression (Adams et al., 2001; Schauben and Frazier, 1995; Sexton, 1999). Psychological effects can include altered religious or spiritual beliefs, changed world views, increased sensitivity to, and fear of, violence, intrusive thoughts, PTSD symptoms, despair and hopelessness, and poor concentration (Dane, 2000; Illiffe and Steed, 2000; Sexton, 1999). When the effects of burnout and vicarious trauma are considered, it is little wonder that practitioners caught in these situations consider leaving their jobs (Barak et al., 2001), with some deciding to change their careers altogether.
Addressing Work Stress
There is much that can be done about work stress, burnout, job dissatisfaction, turnover and their consequences. However, interventions remain the primary responsibility of human service employers rather than employees because the major influences on these factors are within their control. Nevertheless, despite these issues clearly being within the domain of occupational health and safety, responsibility for remedies mostly remains with the individuals directly affected, perhaps reflecting the individualistic orientation of Western society and the advice of some scholars (see Zastrow, 1999).
Organisational Strategies
Despite longstanding and repeated calls for job redesign to address work stress in the human services (Davis-Sachs et al., 1985; Dollard et al., 2001; Poulin, 1994, 1995; Thompson et al., 1996; Winefield et al., 2000), it has not been taken up to any large degree. Indeed, variety and autonomy for many workers have decreased as case management procedures have increased (McDonald, 1999). In view of the plethora of research findings indicating the significant moderating influence of increased worker control and autonomy on burnout, the reluctance of employers to embrace this strategy is surprising. It is fundamentally a management responsibility to establish and maintain an organisational climate and culture that deals openly with work stressors, vicarious trauma and burnout and does not individualise or label those staff who experience these phenomena.
Job redesign would be further enhanced through the proactive use of regular, supportive and good quality professional and administrative supervision (Grasso, 1994; Rauktis and Koeske, 1994; Rycraft, 1994). Management styles that embrace collaborative, participatory approaches that facilitate effective team work and collegial support have been shown to increase job satisfaction and moderate work stress (Smith and Nurston, 1998; Sexton, 1999; Thompson et al., 1996; Zunz, 1998). Sadly though, many managers and supervisors remain unskilled to deal with the social and emotional requirements, or are simply not interested in making this a high organisational or personal priority (Winefield et al., 2000). Similarly, access to debriefing, whilst demonstrated as an effective tool against stressful incidents and vicarious trauma, remains under utilised (Dollard et al., 2001; Illiffe and Steed, 2000).
Organisations have significant roles to play in assisting their staff to manage appropriately and effectively the chaotic situations and stresses that can arise in some human service practice contexts. Having orderly processes and procedures in place can aid the management of work stress but, if overly rigid, can also contribute to it. Staff training in time management, workload planning and prioritising, and how to decrease interpersonal stress and conflict in work teams (eg improved communication) can be very productive. However, this should never be used as a manipulative ploy to shift responsibility for dealing with excessive workloads form the organisation and funding authority to individual practitioners.
Other effective measures to increase job satisfaction and decrease burnout include the provision of challenging and stimulating training (Dollard et al., 1999, 2001), orientations for new workers (Barak et al., 2001), appealing general working conditions including physical surroundings (Dollard et al., 2001; VinokurKaplan, 1991), ensuring there are adequate resources to meet the workload and closely monitoring this (Illiffe and Steed, 2000; Sexton 1999), and addressing financial remuneration issues, which are frequently a key source of worker dissatisfaction (Marriott et al., 1994; Rauktis and Koeske, 1994; Vinokur-Kaplan, 1991). Latting (1991) notes that while the human services attract idealistic practitioners to low paid positions, it is wrong to assume that are not motivated by extrinsic rewards such as salary.
Personal Strategies
There are a number of self-care strategies that social workers and human service practitioners can employ in order to prevent and remedy work stress and vicarious trauma, apart from leaving their positions or occupations. Many of these appear to be common sense, but in practice, with high workloads and the often-superhuman expectations of themselves that many human service workers hold, these measures can be under utilised. Perhaps the most commonly utilised strategy is accessing emotional and instrumental support from one’s personal and professional networks, and supervision. As noted earlier, these are effective responses to dealing with work stress. As the saying goes: A problem shared is a problem halved. However, this assumes that worker are willing to disclose and share their issues with others, but some have been found to prefer to protect their loved ones and others from the distressing events and issues they confront (Illiffe and Steed, 2000; Jayaratne et al., 1986), perhaps leading to less support being proffered.
Emotional distancing has also been cited as a useful, and perhaps necessary, measure to address occupational stress in the human services (Bennett et al., 1993). In essence, it entails workers setting clear boundaries between themselves and their client and work situations in order to prevent themselves being emotionally overwhelmed by the distressing situations in which they often work. This strategy can be enhanced by reflective practice, which involves the worker in a continual process of self-exploration and improvement. Furthermore, some writers suggest that workers will benefit from developing and maintaining a sense of humour and focus on their own spirituality (Sexton, 1999). Practitioners can increase selfawareness and restore a sense of meaning, hope and connection with others through spiritually-oriented activities like meditation, being in nature, prayer and religious activities, existential explorations etc. This can help one to gain perspective about events bigger than oneself (Sexton, 1999). In a similar fashion, positive thinking can be a useful strategy for dealing with stressful events and issues that can eat away at one’s self-esteem and confidence (Zastrow, 1999).
Other self-care strategies include emotional intimacy and sex, which can act as a physical and emotional release and connection with others, and help one to feel well grounded and refreshed. In a similar fashion, relaxation techniques, regular exercise and sporting activities can help workers to release the stress in a healthy and productive way (Dollard et al., 2001; Illiffe and Steed, 2000; Sexton, 1999). Having relaxing times at the movies, concerts, playing or listening to music, sporting events and engaging in pleasurable hobbies can also be productive in handling stress.
Some workers address the workload pressures through planning, goal setting and time-management of their work tasks. This can also facilitate greater variety at work, and if possible and practicable, allow for particularly stressful work to be spaced by less demanding duties. Similarly, being proactive and positive about changing or adapting to distressing events through committed action (eg organisational lobbying, political activity) can prove to be an effective way of addressing the systemic factors and processes that affect the human condition and human service practice (Illiffe and Steed, 2000). These sorts of approaches can militate against feeling powerless in the face of macro events and abuses of power by those in positions of authority. Collective action is a powerful tool for political and social change.

Sample WHS Consultation Procedures
-
Overview
Consultation is mandatory under the Work Health and Safety Act 2011 (WHS Act) for [insert organisation name].
Consultation will take place on all work health and safety matters including:
- undertaking risk management activities
- proposing changes that may affect workers
- making decisions about any work health and safety procedures
- the adequacy of facilities for the welfare of workers
Where [insert organisation name].has concurrent duties under the WHS Act with another PCBU, it will consult, cooperate and coordinate with the other PCBU and its workers, so far as is reasonably practicable.
This procedure should be read with the Work Health and Safety Policy.
-
Considerations
Meaningful consultation can lead to fewer workplace injuries and give everyone the opportunity to:
- discuss and share their health and safety concerns
- identify safety hazards and risks
- find and implement practical solutions
- contribute to the decision making process
- communicate outcomes in a timely manner
-
Procedure Steps
[insert organisation name] consults, so far as is reasonably practicable, with workers who carry out work for [insert organisation name] who are (or are likely to be) directly affected by a work health and safety matter.
If the workers are represented by a health and safety representative, the consultation will involve that representative.
Consultation at [insert organisation name] involves sharing of information, giving workers a reasonable opportunity to express views, and taking those views into account before making decisions on health and safety matters.
[insert organisation name] consults, co-operates and co-ordinates activities with all other PCBUs who have a work health or safety duty in relation to the same matter, so far as is reasonably practicable.
3.1 Health and safety representatives (HSRs)
HSRs may be elected to represent various work groups and investigate health and safety issues.
3.2 Health and Safety Committee (HSC)
An HSC will be established:
- if requested by the HSR, or
- if requested by five or more workers, or
- on the initiative of [insert organisation name].
The role of the HSC is to facilitate cooperation between [insert organisation name] and workers on health and safety matters as well as to develop work health and safety standards, rules and procedures.
3.3 Other Agreed Arrangements
Other agreed arrangements for consultation may be set up by [insert organisation name] provided the arrangement is agreed to by the workers and is likely to result in better consultation and improved decision making.
Once established, consultation must be in accordance with the procedures agreed to between [insert organisation name] and the workers. Regardless of the arrangement, the obligation of [insert organisation name] to consult with all workers remains.
[insert organisation name] may need a mix of HSRs, HSCs and / or other agreed consultation arrangements tailored to suit the workers and [insert organisation name]’s work environment.
[It may be more effective and meaningful to have an alternative arrangement for consultation if workers travel frequently or the CMO s small].
Other agreed arrangements for consultation on health and safety matters used by [insert organisation name] may be through:
- regular scheduled meetings
- team meetings (where work health and safety is always an agenda item)
- one-off meetings
- tool box talks
- regular scheduled meetings
- team meetings (where work health and safety is always an agenda item)
- one-off meetings
- tool box talks
All consultation arrangements will be consistent with [insert organisation name]’s legal duties under the WHS Act.
[insert organisation name] will:
- consult with the workers on how consultation will occur and explain the various mechanisms that are available
- agree on how consultation will take place.
3.4 Nature of consultation about particular matters
[insert organisation name] will ensure:
- that relevant information about the matter is shared with workers, and
- that workers be given a reasonable opportunity:
- to express their views and to raise work health or safety issues in relation to the matter, and
- to contribute to the decision-making process relating to the matter, and
- that the views of workers are taken into account by [insert organisation name], and
- that the workers consulted are advised of the outcome of the consultation in a timely manner.
If the workers are represented by a health and safety representative, the consultation must involve that representative.
3.5 When consultation occurs
[insert organisation name] sets up a plan to ensure that consultation occurs in relation to the following health and safety matters:
- when identifying hazards and assessing risks to health and safety arising from the work carried out or to be carried out by [insert organisation name]
- when making decisions about ways to eliminate or minimise those risks,
- when making decisions about the adequacy of facilities for the welfare of workers,
- when proposing changes that may affect the health or safety of workers, • when making decisions about the procedures for:
- consulting with workers, or
- resolving work health or safety issues at the workplace, or
- monitoring the health of workers, or
- monitoring the conditions at any workplace under the management or control of the person conducting the business or undertaking, or
- providing information and training for workers, or
- when carrying out any other activity prescribed by the regulations for the purposes of this section.
3.6 Consultation Processes
[insert organisation name]:
- sets up consultation processes and
- ensures they are discussed and reinforced regularly and
- documents these processes
- regularly monitors and reviews the consultation procedures to ensure they are
- the most effective form of consultation
[insert organisation name] consults with employees and the Board of Directors on a regular basis, involving them in decision making and informing them of decisions that may affect their health and safety.
Consultative mechanisms include:
- Annual audit of staff meeting minutes and agenda to review WHS items discussed and resolved - this audit will be presented to the Board
- Quarterly inspection of premises and a record of findings, with a roster to ensure all employees are involved in workplace inspection and hazard identification
- Where a new work practice is introduced, employees are consulted and potential and existing hazards reviewed - this information is disseminated to staff as required
- WHS is a standard agenda item Board and staff meetings
Health and Safety Representative [depends on size of CMO] At a minimum, organisations must have an employee with designated responsibility for WHS. Larger organisations may appoint a Health and Safety Representative and should ensure a HS committee remains active, with reporting and follow-up procedures in place. NB: A committee is only mandatory for organisations with over 20 FTE and if requested by staff.
Health and safety committees bring together workers and management to assist in the development and review of health and safety policies and procedures for the workplace.
The functions of the health and safety committee are:
- to facilitate co-operation [insert organisation name] and workers in instigating, developing and carrying out measures designed to ensure the health and safety of workers
- to assist in developing standards, rules and procedures relative to health and safety
- such other functions prescribed by the regulations or agreed between [insert organisation name] and the committee.
The effective operation of a health and safety committee is dependent upon everyone fulfilling their role.
Establishment of health and safety committees
[insert organisation name] must establish a health and safety committee within two months after being requested to do so by:
- a health and safety representative (HSR), or
- five or more workers at the workplace.
A health and safety committee may be established for workers who carry out work at one or more locations or for those who do not have a fixed place of work.
[insert organisation name] may also establish a health and safety committee on its own initiative.
The constitution of the health and safety committee may be agreed to between [insert organisation name], HSR and workers. If agreement is not reached within a reasonable time, any party may ask WorkCover to appoint an inspector to decide the matter.
Health and safety committee membership
The makeup of the committee can be agreed to between the workers and [insert organisation name].
[insert organisation name] can only nominate up to half of the members.
An HSR is a member of the committee if they consent. If there are two or more HSRs at [insert organisation name], then they can choose one or more who consent to be members of the committee.
Calling for nominees
Calling for nominees is an important part of electing a health and safety representative (HSR) in the workplace. All workers can nominate including volunteers.
Once the work groups and number of HSRs required has been agreed, notices calling for nominations should be prominently displayed with a reasonable closing date. They will be in a form that all workers can understand.
Where the number of nominations equals the number of vacant HSR and deputy HSR positions, an election is not required and each candidate is taken to have been elected.
If there are more nominees than positions available then an election will need to be held.
The workers may determine how an election must be conducted (eg by secret ballot or show of hands) however, it must comply with procedures in the draft work health and safety regulations.
If a majority of workers agree, the election may be conducted with the help of a union, other person or organisation.
Electing a health and safety representative
Workers elect the health and safety representative (HSR) from their work group. All workers in a work group are entitled to elect one or more HSRs and deputy HSRs for a three year term.
When agreement on the work groups has been reached, along with the number of work groups and HSRs (and deputy HSRs), [insert organisation name] will provide any reasonable resources, facilities and help to enable an election to be conducted.
After the nominations have been called, an election can be conducted. The members of the work group can determine the election procedure however, there are minimum requirements prescribed in the Work Health and Safety Regulations.
These procedures include that the person conducting the election ensures:
- each PCBU in which a worker in the work group works is informed of the election date as soon as practicable after the date is determined
- all workers in the work group being given an opportunity to:
- nominate for the position of HSR
- vote in the election
- all workers in the workgroup and all relevant PCBUs are informed of the outcome of the election.
Operation of health and safety committees
The [insert organisation name] health and safety committee (HSC) must meet at least every three months and at any reasonable time when requested by at least half the members of the committee.
[insert organisation name]supports members of the HSC by allowing them:
- reasonable time to attend meetings and carry out their functions as a committee member, and be paid at their normal rate of pay when doing so
- access to information about hazards and risks at the workplace as well as information relating to the health and safety of workers at the workplace (excluding workers’ personal medical information without the workers' consent)
- opportunities to develop skills relevant to their role on the HSC.
The role of workers on HSCs is to ensure genuine worker representation in health and safety matters that affect them.
Work groups
Work groups are workers represented by a health and safety representative (HSR).
Usually these workers perform similar types of work and have similar health and safety concerns and conditions within the workplace.
Work groups allow workers' interests to be represented effectively and conveniently.
The purpose of workers belonging to a work group is to facilitate representation on work health and safety matters by an HSR.
Once an election for an HSR has been requested [insert organisation name] must start negotiations with workers within 14 days to establish work groups.
This process will also help [insert organisation name] and workers in a work group negotiate the number of HSRs and work groups required.
Determining work groups
In determining work groups, [insert organisation name] considers:
- the number of workers
- the views of workers in relation to the determination and variation of work groups
- the nature of each type of work carried out by the workers
- the number and grouping of workers who carry out the same or similar types of work
- the areas or places where each type of work is carried out
- the extent to which any worker must move from place to place while at work
- the diversity of workers and their work
- • the nature of any hazards at the workplace or workplaces
- the nature of any risks to health and safety at the workplace or workplaces
- the nature of the engagement of each worker, for example as an employee or as a contractor
- the pattern of work carried out by workers, for example whether the work is full-time, part-time, casual or short-term
- the times at which work is carried out
- any arrangements at the workplace or workplaces relating to overtime or shiftwork.
Decisions about establishing work groups must be made by consultation and agreement between [insert organisation name] and the relevant workers. A worker’s representative can be appointed by the workers to negotiate on their behalf.
A work group may involve multiple CMOs (&/or other PCBUs) at one or more workplaces and these are called multiple business work groups. The aim is to identify the most workable arrangement for the workplace. When agreement on the work groups has been reached, [insert organisation name] must notify the workers of the outcome of the negotiation.
Multiple business work groups
Multiple business work groups may be agreed with workers carrying out work for two or more CMOs (&/or other PCBUs) at one or more workplaces. The work group arrangement must be agreed to by the workers.
The aim is to identify the most workable arrangement for the workplace/s
Determination of work groups of multiple businesses
Multiple business work groups must be determined by negotiation and agreement between each of the CMOs (&/or other PCBUs) and the workers.
The determination of multiple business work groups need not affect pre-existing work groups or prevent the formation of additional work groups.
Negotiations will be focused on:
- the business or undertaking to which the work groups will apply
- the workplace location/s of work groups
- the number and composition of work groups
- the number of HSRs and deputy HSRs.

PART I: Types of Health and Safety Training
There are many health and safety training courses available. As an employer, it is crucial that the 'training product' you buy suits your staff and your business.
Formal Training
Types of Formal Training Programs and Courses
There are basically four types of health and safety training courses available:
- Licence or certificate courses
- Accredited and approved courses
- Short courses
- Vocational and professional courses
Types of Formal Training Courses
Licence or Certificate Courses
Certain jobs require an operator to hold an officially recognised certificate or licence to do tasks like operating a steam boiler, driving a crane or working as a dogman on a construction site.
Training for these certificates or licences in most States and Territories is provided by an accredited trainer and assessment is carried out by a qualified assessor.
Assessment can take place either at work or a place where training is conducted (eg a skills centre). The health and safety organisation in your State or Territory can advise you on these training programs.
Accredited and Approved Courses
Courses like introductory training courses for health and safety representatives are classified as accredited under legislation. Some States and Territories use the term approved for these courses. Courses for managers and supervisors may also be classified as accredited in some States and Territories.
Accredited and approved courses have to meet certain criteria determined by the relevant Commonwealth, State or Territory health and safety authorities.
Short courses
Short courses are usually designed for a specific group of people such as operators of equipment, employees, managers and supervisors. The most common types of short courses are:
- General introductory courses on topics such as hazard management
- Management and supervisory training courses on legal obligations and managing health and safety in the workplace
- Courses on specific issues such as hazardous substances, manual handling, confined spaces and workplace ergonomics
- Courses for employees with non-English-speaking backgrounds giving a general introduction to basic health and safety principles
Vocational and professional courses
Traineeship and apprenticeship courses normally include health and safety modules as part of the course.
There are also 2 to 4 year health and safety courses for training health and safety professionals and managers. These courses usually involve part-time study at a college or university over 2 to 4 years and result in a qualification in health and safety.
Arrangements for accrediting and approving OHS trainers and training courses are different in each State and Territory. Check with the OHS organisation in your State or Territory for specific information (see page 29 for contact details).
Who Can Provide Training?
Most health and safety training is provided by:
- Employer organisations
- Unions
- The health and safety organisation in your State or Territory or the Commonwealth sector
- TAFE colleges and universities
- Private occupational health and safety consultants/trainers
Many employers send their supervisors to these organisations for training. Training can also be provided in-house by these organisations.
Informal Training
The Role of The Supervisor or Experienced Worker
Another important provider of training may be a supervisor or experienced worker who has skills and knowledge in health and safety. Such a person can provide information and training to others at work.
For this informal training to be effective, the supervisor or experienced worker needs to undertake trainer-training to develop the skills to train others in the workplace.
Your local TAFE college, private training providers and the trade unions may offer trainer-training courses which generally run for 3 to 5 days.
When Do People Need Health and Safety Training?
The need for health and safety training at work is continuous. As circumstances at work change, there will always be the need to ask the questions:
- How does this change affect health and safety?
- What health and safety instruction and training do I need to provide now?
Typical times when you need to ask these questions are:
- Whenever you take on someone new at work - health and safety is an important part of induction training
- Whenever you buy new machinery or equipment or new substances such as cleaning materials, chemicals, paints and so on
- Whenever people's jobs change n whenever you change the layout of your work environment
- Whenever there are new health and safety regulations, standards or laws that affect your industry
- If there has been an accident, injury or health and safety incident at work
How Do You Select the Training That Meets Your Needs?
First, you need to make decisions about the amount of money and time you want to invest in training.
It is useful to ask other employers what they think of the health and safety training providers they have used. You may also want to ask training providers about how flexible they can be and what sort of service they can provide to you.
Decisions You Need to Make
- How much money are you going to invest in training over the next 6 to 12 months?
- How much time will you devote to training?
- What is the most cost efficient way for you to make this investment?
- To send one employee to the health and safety course and a train the-trainer course and then schedule time for him/her to train others at work?
- To send a group of people to the training course?
- To arrange for a trainer to come to the work site and deliver training to a group of workers?
- What specific outcomes do you want to achieve as a result of the health and safety training?
Health and Safety Skills and Knowledge at Work
What health and safety skills and knowledge do people at work need? This section looks at induction training, planning training and doing a training needs analysis, and the health and safety responsibilities of the employer/manager, the supervisor and the employee.
Who Needs Health and Safety Training?
In all organisations, no matter how large or small, everyone needs some training in health and safety matters:
- The employer
- The supervisor
- All employees - casual, part-time and full-time
- Students on work experience
- New employees
- Contractors who work on your site
- The health and safety committee representative
- Members of the health and safety committee
What Training Does Each Person Need?
The type of training that each person in the organisation needs depends on:
- Each person's role and responsibilities at work
- Each person's occupation (eg plant and machine operators and people who handle hazardous substances need specific training)
- The hazards identified during an inspection of your workplace
- The type and occurrence of injury and disease at work
The Importance of Induction Training
Whenever someone new starts work, the employer is responsible for providing induction training. Induction training is needed by all new employees – whether they are full-time, part-time, casual or even volunteers on site or students doing work experience.
Induction to Health and Safety
Induction training must include providing health and safety information such as:
- Hazards at work
- How to interpret safety signs and information
- How to work safely and use equipment safely
- Fire and emergency procedures
- First aid procedures
- Who to report incidents or accidents to
- Who to discuss safety issues with
- How to get involved in health and safety
Who Provides Induction Training?
The employer is responsible for ensuring that a new employee or trainee is given induction training and has the skills and knowledge to work safely. In most workplaces the owner, supervisor or experienced worker will provide this training.
Keeping Records of Induction Training
It is also the employer's responsibility to keep records of induction training. The person in charge of providing induction training should keep records of the following types of information:
- Name of the person who received induction health and safety training
- Dates and times when the training was provided
- Specific details of what was covered during the training sessions
- How long the training sessions lasted
- How the training was assessed
Planning Training and Training Needs Analysis
Training programs are best planned if everyone at work:
- Has basic information about what the laws and regulations are
- Has the opportunity to talk about health and safety concerns
- Uses the health and safety skills and knowledge they have
- Takes part in a workplace inspection and identifies hazards at work
- Takes part in a training needs analysis to find out what training each person needs
Training Needs Analysis
Conducting a health and safety training needs analysis will help to ensure that the people in your organisation get the type of training they need.
It will enable you to ensure that the training is relevant to the job and the changing needs of the workplace.
A training needs analysis involves analysing all aspects of work, including the work environment, the actual jobs people do and the skills and knowledge of each person at work. Once this information is collected, then you can start to plan what training your organisation needs.
There are a number of stages to a training needs analysis, as described below.
Training Needs Chart
Appendix 1 [Part II of this reading] contains a chart to help you start planning the training you need to organise for yourself and your employees. Discuss the plan with your employees.
Stages of a Training Needs Analysis
- Analyse the workplace. This means analysing:
- the working environment
- the activities that people are expected to perform at work
- Assess the current approach to health and safety at work. This may include looking at:
- selection and recruitment procedures
- the way jobs are designed
- the way equipment and tools are selected
- the way work procedures are designed and managed
- Analyse jobs. This means studying a job and identifying all the tasks, equipment, materials, work processes and the associated hazards.
- Forecast job changes. This means making predictions about the way jobs may change and how changes may affect the health and safety of staff.
- Identify the skills, knowledge and attitudes needed to prevent health and safety problems
- Assess the current situation. This means:
- identifying the actual health and safety competencies that people in the organisation already have
- comparing these existing competencies to those needed to prevent health and safety problems
- working out deficiencies which health and safety training would reduce or eliminate
PART II: Appendix 1

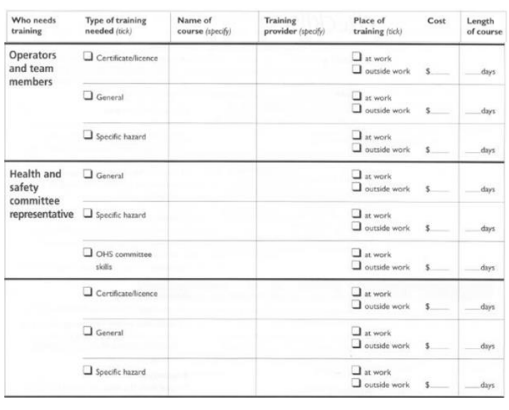
Appendix 2
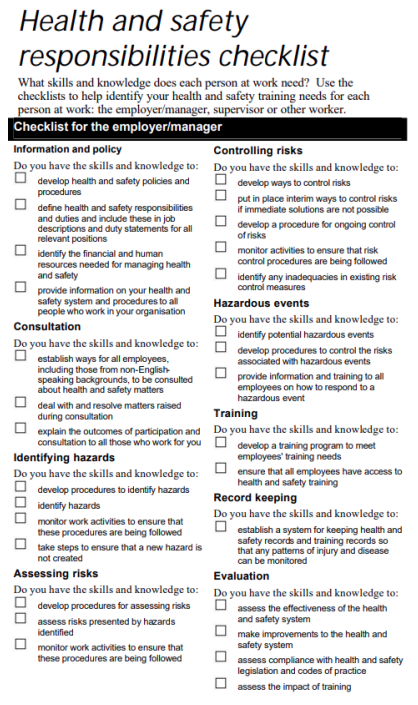
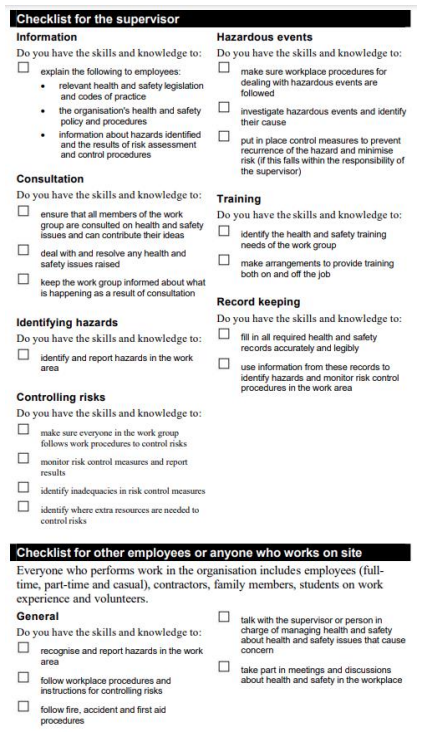

Maintain health and safety records and statistics and keep all your written health and safety records organised and available for reference.
Employers are required to keep health and safety records and statistics on file. Examples of documentation include training activities, first aid treatments, and incident investigations.
Written records and statistics can help to:
- identify trends for unsafe conditions or work practices so you can take steps to correct these potential hazards;
- provide material for education and training; and
- provide documentation in case it is requested or if an incident occurs and you need to prove that you did all you could reasonably do to prevent it.
Records and statistics that should be maintained include:
- records of consultation on safety matters with your workers;
- health and safety program reviews can help you track the progress of the program;
- worker orientation records that can help ensure that workers are getting the education and training they need;
- inspection reports can provide historical information about hazards a business has encountered and how you have dealt with;
- monthly meeting records that can help monitor how promptly and how well action items have been carried out;
- incident investigation reports that can clarify which hazards have caused incidents and how they were controlled;
- first aid assessments that can help determine the first aid requirements for the workplace; and
- first aid records that can provide injury statistics that will help prioritise health and safety efforts.
Statistics that may be of value include the:
- number of incidents and injuries each year;
- number of workdays lost each year; and
- cost to the business from workplace injuries each year

-
Introduction
The University of Wollongong acknowledges that guidelines on incident management are an essential component of the workplace health and safety management system. The provision of timely and efficient first aid and medical response is crucial in caring for staff, students and visitors in the event of an injury. Additionally, timely and efficient reporting on hazards, incidents and other occurrences with an adverse risk to health and safety are required to be in place so that risk assessment and appropriate corrective action can be taken.
These guidelines should be read in conjunction with the following:
- First Aid Guidelines
- WHS Risk Management Guidelines
- Injury Management Program
- Emergency Management Procedures.
-
Scope
This document sets out the procedures for the management of an incident requiring first aid or medical treatment for injuries which occur to University staff, students or visitors. This includes University activities which occur on or off campus.
This document also describes the University’s internal and external reporting process for injuries, illnesses, incidents, health and safety hazards, dangerous incidents and system failures.
-
Definitions
- Biohazard. A biohazard can be defined as any organism (and/or its toxin) or a material of biological origin that can cause harm to human, plants, animal or the environment.
- Dangerous Incident. Imminent risk of the death of, or serious injury to, anyone; an incident that endangers or is likely to endanger the safety of people at a workplace.
- First Aid. Initial treatment for an injury which is normally given by a first aider
- First Aid Officer. Person nominated to administer first aid at the University; must hold a current Provide First Aid Certificate.
- Hazard. A source or a situation with a potential for harm in terms of human injury or ill-health, damage to property, damage to the environment, or a combination of these.
- Hazard Identification. The process of recognizing that a hazard exists and defining its characteristics
- Illness. Any physical or mental ailment, disorder, defect or morbid condition which can be of sudden or gradual development. This also includes the aggravation, acceleration, exacerbation or recurrence of any preexisting disease.
- Incident. Any unplanned event resulting in, or having a potential for injury, ill health, damage or other loss.
- Injury. Any physical or mental damage to the body caused by exposure to a hazard.
- Lost Time Injury. A work related injury which results in a person being absent from work for at least one full shift.
- Medical Treatment Injury. A work related injury which results in treatment provided by a qualified health professional e.g. General Practitioner, Physiotherapist.
- Near Miss. An incident that does not produce an injury or disease but has the potential to do so.
- Risk. The likelihood and consequence of an injury or harm occurring
- Risk Assessment. The process of estimating the magnitude of risk for an activity and identifying the actions to take to eliminate or minimise the risk.
- System Failure. When a system fails to meet its requirements.
-
Responsibilities
4.1. Workers and Students
Workers and students are responsible for the following:
4.2. Supervisors and Managers
Supervisors and Managers are responsible for the following:
4.3. WHS Unit
The WHS Unit is responsible for:
- reporting hazards, incidents, injuries, dangerous incidents and systems failures which occur or have the potential to occur, and
- in the event of an injury or unsafe situation, do what they can to ensure the safety of others
- ensuring that injured workers, students or visitors to the University receive, or is referred to, appropriate first aid &/or medical assessment for any reported injury/illness
- immediate referral to the WHS Unit of any injured worker, student or visitors to the University who require medical assessment or treatment
- hazards, incidents, injuries, dangerous incidents and systems failures are appropriately reported for areas under their supervision
- corrective actions are developed in consultation with workers and students and are implemented to eliminate the risk of injury, or where this is not possible, reduce the risk to an acceptable level
- follow up on the effectiveness of implemented corrective actions in consultation with workers and students
- monitoring and reviewing the system for effective incident management and reporting
- providing advice and recommendations to local areas on preventative and corrective action to improve the level of health and safety
- conducting investigations and follow up of significant incidents to prevent reoccurrence, in line with the Incident Investigation Procedure.
-
Incident Management Procedure
5.1. Scene Preservation
In the case of a ‘notifiable incident’, the scene of the hazard, incident or injury cannot be disturbed. A ‘notifiable incident’ under the Work Health and Safety (WHS) Act 2011 relates to:
The site where the incident occurred must not be disturbed in any way, other than to assist an injured person or make the area safe, until such time as a SafeWork NSW inspector arrives at the site or any earlier time that an inspector directs.
Further information can be found in 7 External Reporting Procedures.
5.2. Immediate Action
Depending on the risk of the hazard or incident involved immediate action must be taken to prevent further persons from being injured. This may involve the activation of emergency procedures or other actions to control the immediate risk to persons in the area, e.g. barricading the area, alerting Facilities Management (or equivalent), Security or the WHS Unit.
5.3. First Aid and Medical Assistance
The flowchart on the following page outlines the process for obtaining first aid and medical assistance on the Wollongong Campus. Clarification on the process is outlined further in this section.
*Security will direct ambulance to the location of the injury. Emergency services are to be contacted directly for life-threatening situations who may be able to provide immediate response procedures.
For campuses other than Wollongong, please refer to the appropriate emergency contact details in Appendix 1: Satellite Campus Emergency Contact Numbers.

5.4. Assessing the Need for Medical Treatment
In most cases the need for medical treatment after an injury is obvious. The following list of injuries and symptoms, although not exhaustive, provides guidance on when to refer to medical treatment:
In some circumstances the need for medical treatment may not be obvious – examples include:
5.5. Medical Treatment
Medical treatment can be obtained by contacting Security on 4221 4900 (ext 4900) at the Wollongong Campus. Refer to Appendix 1: Satellite Campus Emergency Contact Numbers for nonWollongong campuses). Alternatively, Emergency Services can be contacted directly on ‘000’ (dial 0 from a University landline phone for an outside line) to arrange for an ambulance to arrive at the scene of the incident.
In some cases, it may be appropriate to transport the injured person to a medical centre for treatment. Where this is the case, the injured person should be referred to one of the following medical treatment centres dependent upon availability and expertise:
This should be decided on a case-by-case basis in consultation with the injured person by the attending first aid officer or the Injury Management Coordinator. For example a swollen ankle may be treated more promptly at a local medical centre as opposed to raising an ambulance. If in doubt contact the Injury Management Coordinator on ph: 4221 5907.
For injuries occurring at campuses other than Wollongong, the injured should be referred to the nearest general practitioner, medical centre or hospital if an ambulance is not required.
- the death of a person
- a serious injury or illness of a person (see Appendix 2: Serious Injury or Illness Table), or
- a potentially dangerous incident.
- heart attack
- stroke
- shock
- epilepsy and seizures – if abnormal or severe
- hyperglycaemia or hypoglycaemia – if abnormal or severe
- burns larger than 20 cent piece, electrical burn • lacerations - if bleeding is severe or persistent
- soft tissues injuries, e.g. sprains and strains
- dislocations and fractures
- head, neck and spinal injuries
- facial injuries
- poisoning
- bites and stings
- overexposure to extreme environmental temperatures
- asthma attack
- electric shock
- loss of consciousness
- overexposure to radiation or hazardous chemicals
- after an electric shock - any person who has received an electric shock, no matter how minor it may seem, should be assessed by a medical practitioner as there could be delayed affects such as an irregular or lower heart rate
- after recovering from unconsciousness - any person who has lost consciousness, even for a small amount of time, should be assessed by a medical practitioner.
- IOH, 32 Swan St Wollongong, ph 4229 6111
- CS Health, 558-580 Princes Hwy Woonona, ph 4286 5400A
- Campus Clinic, UniCentre Building 11, ph 8203 5901, or
- the injured person’s general practitioner
-
Critical Incidents
Critical incidents are those which directly or indirectly cause significant distress to a person, either at the time it occurs or later. A critical incident may require the activation of emergency procedures.
The following options are available for support and assistance for those experiencing critical incident distress:
- University Employee Assistance Program [Optum]: This is a professional counselling service available to University staff or their families which is confidential and free for personal or work related problems. This service is voluntary and provided by experienced registered psychologists and counsellors. To access the University EAP contact Optum directly on 1300 361 008.
- Student Counselling: The University offers a free and confidential service available to postgraduate and undergraduate students with personal, work or study related difficulties. Counsellors are experienced registered psychologists. To access Student Counselling contact the Counselling Services Unit on 4221 3445.
-
Internal Incident Reporting Requirements
The following outlines the process for the internal reporting of incidents including health and safety hazards, injuries, illnesses, dangerous incidents, near-misses and system failures.
In some instances, notification to the WHS Unit is required immediately after an incident has occurred or hazard is identified. Occasions where this may occur include:
7.1. Types of Incidents to be Reported
The list below represents general criteria for the type of incidents to be reported using the SafetyNet report form. The list is not meant to be exhaustive and may require tailoring to specific areas:
- when a hazard is identified which poses an immediate risk to health and safety, or
- an injury which requires medical treatment (does not include first aid), or
- time lost from work, or
- ‘notifiable incidents’ as defined in Section 7 External Reporting Procedures
- any injury to staff, students, contractors or visitors of any nature or severity sustained whilst on University campus or whilst undertaking a University activity off campus e.g. field trip, approved travel, clinical work, attendance to conferences, student placement etc
- any incidents which may have had the potential to cause an injury, including diseases in animals that have the potential to be transferred to humans, exposure to chemical agents or physical agents, genetically modified organisms, imported biological materials, radiation or other hazards
- dangerous incidents or system failure which caused or had the potential to cause serious property damage e.g. fires, floods and explosions
- all vehicle accidents occurring on University grounds or whilst conducting University business • any injury or incident to staff sustained whilst travelling to or from the University (Journey claims) • sporting injuries arising from University organised activities, both formal and informal
- injuries sustained by staff or students participating in University organised social activities.
-
Hazard/Incident Report Form
A SafetyNet hazard/incident report is to be completed for all hazards, incidents, injuries, illnesses, dangerous incidents and system failures arising from reported hazard, incidents or workplace safety inspections as outlined in 6.1 Types of Incidents to be Reported. Further information on using SafetyNet is available in the SafetyNet User Guide.
8.1. Submitting the Hazard/Incident Report Form
Once the online report form has been submitted a copy is sent to the nominated supervisor for approval and the WHS Unit for review.
8.2. Incident description
The details of the incident should be factual and relevant. Describe the details of the incident as clearly as possible. This should include the exact time and place of the incident, the circumstances which led up to it, the sequence of events in the incident itself, the number of people involved, and the names and contact information of any witnesses present.
8.3. Contributing factors
When trying to determine corrective actions to prevent reoccurrence, it is helpful to analyse the contributing factors that led to the incident occurring. A list of possible contributing factors is divided into four categories listed below:
8.4. Cause
Determine the cause of the incident e.g. what lead to the incident occurring? If this cause was removed or was not present, would this incident still happen?
8.5. Risk level
Identify the level of risk of the incident taking into account likelihood and consequence with current controls in place. The risk score determines the priorities for corrective actions to be implemented.
8.6. Corrective Actions
The implementation of appropriate corrective actions is critical to the success of reducing the risk of hazards in the workplace.
Corrective actions should be specific, measurable, achievable, relevant, and time-related (SMART). From the risk assessment, corrective actions will need to be implemented to eliminate or reduce the risk to an acceptable level utilising the hierarchy of controls. If longer-term corrective actions are chosen (eg those involving high cost or requiring lengthy manufacturing time and complex approvals) then lower level corrective actions should be temporarily implemented.
Corrective actions should:
Corrective actions may not only involve process control measures but also address system deficiencies in the WHS management system.
Depending on the risk of the hazard involved, the following time periods will be used as a guide for the prioritisation and completion of corrective actions:
- Design - Design factors include faults with the design of plant, equipment or work practices.
- Behavioural - Behavioural factors relate to human aspects which can sometimes lead to an incident.
- Environmental - Environmental factors relate to the surroundings of a workplace and whether they led to the incident occurring.
- System - System factors include procedures etc which need to be changed to prevent reoccurrence.
- be determined in consultation with workers who will be directly affected by the implementation of the corrective actions in the workplace
- be implemented in a timely manner as per the WHS Risk Management Guidelines
- be appropriate for the root cause
- control the hazard and risk to an acceptable level • not introduce a new hazard or risk (or if they do, ensure this new hazard or risk is assessed).
| Risk Level | Corrective Action Time Frame | Priority Level |
|---|---|---|
| High | As soon as possible, but not longer than 24 hours | 1 |
| Medium | 14 days | 2 |
| Low | 28 days | 3 |
At least one corrective action is required to be implemented to reduce the risk to an acceptable level.
Once the corrective action plan is determined, including responsibilities and timeframes, is the details are to be recorded in SafetyNet. On approval by the supervisor, risk control methods (corrective actions) detailed in the report form will be emailed to the nominated party for action. Corrective actions are communicated and monitored via email. Once a corrective action has been completed, the date of completion is entered for the incident as listed in the responsible person’s work-list on SafetyNet.
If corrective actions are not completed by their due date reminder emails are sent to the responsible person. Corrective actions which are not completed on time are reviewed by the WHS Unit on a monthly basis and escalated to the nominated supervisor to outline a plan for completion.
If there is any doubt on the unit responsible for undertaking a corrective action please liaise with the WHS Unit on 4221 3931 (ext 3931). The WHS Unit will consult with the person reporting the incident and seek to identify the responsible unit for the issue and the workers and supervisor of the area(s) involved to ensure appropriate ownership of the corrective action. In the rare case of a dispute with regards to the responsibility of corrective actions, the dispute is to be raised in writing to the Manager WHS who will assist with the appropriate assignment of corrective actions following review of the hazard and incident report.
-
Review
Follow up of the implementation of the controls should be conducted by the supervisor to ensure the following questions are answered:
If required another hazard report may be required to document a new hazard or initiate further corrective actions.
- have the corrective actions as stated by the initial notification been completed?
- has the corrective actions as stated in the initial notification been effective in reducing the risk of injury?
- has the corrective actions introduced new hazards?
-
External Reporting Procedures
Incidents which are required to be notified to SafeWork NSW, including employees, students, contractors or visitors, shall be completed by the WHS Unit once notified by the supervisor.
The WHS Act 2011 creates a duty on persons conducting a business or undertaking to notify SafeWork NSW immediately after becoming aware that a notifiable incident arising out of the conduct of the business or undertaking has occurred.
A ‘notifiable incident’ means:
Further information is available on SafeWork NSW’s Notifying Us web page and WHS Incident Notification: Fact Sheet. In addition, notification is required of any incident in relation to a workplace that exposes a worker or any other person to a serious risk to a person’s health and safety emanating from an immediate or imminent exposure to:
Incidents involving Genetically Modified Organisms (GMOs) should be reported immediately to the WHS Unit and the University’s Gene Technology Review Committee (GTRC). The Office of Gene Technology (OGTR) will be notified as soon as practicable by the Chair of the GTRC.
Incidents involving imported materials should be reported to Department of Agriculture & Water Resources. Refer to the University’s Biosafety Manual for further details.
Incidents involving ionising radiation shall be reported to the NSW Environmental Protection Agency (EPA) as per the Radiation Safety Guidelines.
- the death of a person, or
- a serious injury or illness of a person (see Appendix 2: Serious Injury or Illness Table), or
- a dangerous incident.
- an uncontrolled escape, spillage or leakage of a substance, or
- an uncontrolled implosion, explosion or fire, or
- an uncontrolled escape of gas or steam, or
- an uncontrolled escape of a pressurised substance, or
- electric shock,
- examples of electrical shock that are NOT notifiable:
- shock due to static electricity
- extra low voltage' shock (i.e. arising from electrical equipment less than or equal to 50V AC and less than or equal to 120V DC)
- defibrillators are used deliberately to shock a person for first aid or medical reasons,
- examples of electrical shocks that are notifiable
- minor shock resulting from direct contact with exposed live electrical parts (other than 'extra low voltage') including shock from capacitive discharge
- examples of electrical shock that are NOT notifiable:
- the fall or release from a height of any plant, substance or thing, or
- the collapse, overturning, failure or malfunction of, or damage to, any plant that is required to be design or item registered under the WHS Regulations, or
- the collapse or partial collapse of a structure, or
- the collapse or failure of an excavation or of any shoring supporting an excavation, or
- the inrush of water, mud or gas in workings, in an underground excavation or tunnel, or
- the interruption of the main system of ventilation in an underground excavation or tunnel.
-
Incident Investigation
The nature of the incident will determine the level of investigation required. Incidents are classified into 3 levels to determine the appropriate level of investigation response:
11.1. Level 1 Investigation
Level 1 incidents are those which have a lower level of risk and are not categorised as being notifiable to SafeWork NSW. Examples of Level 1 incidents may include:
Level 1 incidents require the operational line e.g. line managers, supervisors, workers, to review the details of the incident, identify possible contributing factors, provide a cause of the incident, assessing the risk of the hazard and implement appropriate corrective actions. The outcome of Level 1 incident investigation shall be recorded on the SafetyNet hazard/incident report online form.
Knowledge of these guidelines shall form the basis of competency for completing level 1 investigations.
NOTE: The WHS Unit may deem any level 1 incident to require a level 2 investigation if there is reason to believe that a detailed investigation is required.
11.2. Level 2 and 3 Investigation

The WHS Unit conducts Level 2 and 3 investigations in accordance with the Incident Investigation Procedure.
Level 2 and 3 incidents have a higher level of risk and are categorised as being notifiable to SafeWork Level 2 and 3 incidents have a higher level of risk and are categorised as being notifiable to SafeWork
Where a Level 1 incident is reported through SafetyNet and is rated as ‘High’, a copy of the report will be communicated to the Executive Dean, Head of School and Faculty Executive Manager. A Level 2 investigation will be conducted.
- Level 1 - Incidents are those which are lower level risks and are not categorised as being immediately notifiable to SafeWork NSW
- Level 2 - Incidents are those which constitute notification to SafeWork NSW but not immediate
- Level 3 - Incidents require prompt notification and investigation by SafeWork NSW or other external agencies. The investigation response required for each level is outlined below.
- first aid injuries
- injuries which may require minor medical treatment
- identified hazards which do not present a serious risk of injury
- minor property damage
- minor environmental damage.
-
Privacy and Confidentiality
Any incident reported as a requirement of this guideline will be handled in confidence in accordance with the UOW Privacy Policy.
Medical information received via incident reports will be treated as confidential. Any names or other identifiers included in SafetyNet reports will be removed to preserve confidentiality of the injured person by the WHS Unit.
-
Related Documents
- Biosafety Manual
- Emergency Management Procedures
- Emergency Procedures Guide
- First Aid Guidelines
- Incident Investigation Procedure
- Privacy Policy
- SafetyNet User Guide
- WHS Unit SOP SafetyNet Reporting Procedure
-
Reference Documents
- WHS Act 2011
- WHS Regulation 2011
- Notifying Us (SafeWork NSW)
- WHS Incident Notification: Fact Sheet (SafeWork NSW)


Under the Work Health and Safety Act 2012 (SA), a Person Conducting a Business or Undertaking (PCBU) must ensure, so far as is reasonably practicable, that workers are safe from injury and risks while at work. This requires safe systems of work to be in place.
Should a workplace incident or injury occur, the PCBU must investigate it to find the cause and to avoid it happening again: not apportion blame. The function of an investigation is to establish all the factors involved in the incident and determine appropriate action/s to prevent a recurrence.
Risk Control Measures
The risk management processes outlined in the Code of Practice – How to Manage Work Health and Safety Risks should be used to identify and control risks.
The risk management process involves four steps:
- Identify hazards – find out what could cause harm.
- Assess risks, if necessary – understand the harm that could be caused by the hazard, how serious it could be and the likelihood of it happening.
- Control risks – implement the most effective control measures for the circumstances.
- Review control measures – to ensure they are working as planned and revise as necessary to make sure they work as planned. This is especially important following an incident.
Investigation Procedure
As a first priority, ensure that any person who has sustained an injury has received appropriate first aid or medical attention.
Secure the scene, make the incident area safe and keep people not providing immediate and urgent assistance away from it.
The scene of an incident should remain undisturbed until all of the facts are collected. Check with a SafeWork SA Inspector before removing anything from the scene for further examination and analysis.
If there has been a death or serious injury, the site should not be altered in any way without the permission of a SafeWork SA Inspector or police officer. Co-operate with emergency services personnel, SafeWork SA Inspectors and specialists taking evidence or measurements.
Incident Notification
The Work Health and Safety Act 2012 (SA) requires PCBUs to notify SafeWork SA of fatalities, serious injuries and illnesses, as well as dangerous incidents that arise, as soon as they become aware of the incident. This is a legal obligation.
All serious work-related injuries and incidents must be reported to SafeWork SA by telephoning 1800 777 209 (statewide – 24 hours). In some circumstances, SafeWork SA may ask for confirmation of details to be provided in writing within 48 hours.
If you are unsure whether or not to report any workrelated injuries or incidents to SafeWork SA, contact the SafeWork SA Help Centre on 1300 365 255.
SafeWork SA may also conduct an investigation of any incident.
Recording and Gathering Information
Record physical evidence first. Physical evidence may be subject to rapid change or obliteration and should therefore be the first information recorded.
Collect and photograph information such as:
- location of the injured worker(s) at the time of the incident
- equipment in use at the time
- substances in use at the time
- safety devices or controls used at the time
- position of appropriate guards
- position of controls for any machinery involved
- damage to equipment
- state of housekeeping in the area
- environmental conditions e.g. weather, lighting, noise levels, temperature.
Take notes of the scene. Photographs, sketches and diagrams may also be useful. Careful study of these later may reveal conditions or contributing factors initially missed.
Take notes about:
-
Events leading up to the incident
- systems of work being used
- instructions given, any variations from instructions
- workplace conditions e.g. lighting, housekeeping, floor surfaces, stair treads, handrails, temperature
- the exact location of the incident
- any materials being used or handled
- the type of transport or equipment being used
- any information at all which may provide clues about contributory factors
-
The incident itself
- the state of the system and the actions that occurred at the moment of the incident
- the person(s) directly involved and those involved at a distance
- the tools, equipment, materials and fixtures directly involved.
-
What happened after the incident
- the injuries/damage which directly resulted
- the events leading to consequential injury or damage
- the persons involved, including those who rendered first aid
- any problems dealing with injuries or damage
Gather the procedures and safety requirements for the area and tasks being performed. Compile a maintenance history of any plant or equipment involved.
Review all potentially useful information about the workplace, equipment and procedures, including designs, specifications, drawings, and information from manufacturers and suppliers.
Interviews
Personally interview everyone involved, including the injured worker(s) if possible, witnesses, nearby workers and anyone in the area at the time. Conduct interviews as soon as possible after the incident.
Interview each person separately. Put them at ease and approach the interview in a non-threatening and non-judgemental manner. Explain that the purpose of the investigation is to prevent a recurrence and identify underlying causes. Ask each person to describe what they saw and heard leading up to and at the time of the incident. Let the person talk without interrupting them.
Ask open ended and probing questions to fill in the details e.g. “Could you expand on this process?” or “Can you tell me about the operation of the equipment?”.
Confirm that your understanding of the person’s account is accurate. End the interview on a positive note, thanking them for the information provided. Ask them to let you know if they recall anything further that may assist.
Reporting and Follow-up
Analyse the investigation details gathered and write a report that can be acted upon to control the identified risks and hazards.
Other Information to Record
-
PCBU and workplace
- PCBU name
- Industry of PCBU
- PCBU location
- Recording Unit (identification of workplace location where incident occurred)
- Work Health and Safety Committee
- Number of workers
- Number of hours worked
-
Person(s) involved in the incident
- Personal characteristics
- Name of injured worker
- Gender
- Date of birth
- Preferred language
- Basis of employment
- Shift arrangements
- Full-time/part-time, permanency of employment
- Employment arrangements
- Job characteristics
- Occupation
- Experience in task Proportion of shift worked
-
Incident details
- Date of incident or report of disease
- Time of incident
- Training provided
- Description of incident Cause of incident
-
Outcome of injury or disease
- Preventative action proposed and taken
- Rehabilitation status
- Fatality, injury, permanency Resumption of work
- Time lost from work
- Nature of injury or disease
- Bodily location or injury or disease

Evaluating performance is only one step on the path to improving performance. While it is possible to use in-house experience and external expertise such as consultants to further improve, some organisations use the process of benchmarking themselves against others. In this way, they may hope to speed up the learning process.
Benchmarking Between Organisations
Benchmarking allows you to assess the activities and service performance of your enterprise against those who have attained best practice. The most useful form of HS benchmarking is qualitative, involving processes and procedures. By contract, numerical or quantitative benchmarking – for example, comparing outcome figures or rates (LTIFRs) – may show areas for improvement but not how to get there. That requires people to analyse the way they carry out work, setting out the steps, tools, time, standards and so on. For example, the activity of handling compensation cases can be quite intensive and costly, making it a good candidate for benchmarking with those who have a reputation for excellence. To analyse the activity accurately requires training in techniques such as process flow-charting and cause-and-effect analysis (fishbone charts) and various problem-solving tools.
The scope of HS benchmarking may be big – the entire WHS management system – or small as in the case of compensation. Newcomers are advised to start with a small project to develop an understanding of the issues and build confidence. Management is more likely to endorse a gradual approach as the process requires time and resources. It will also want to see a return and that means careful identification of those projects that will have a recognisable impact. Eventually, it could be applied to HS in mainstream areas such as maintenance, training, purchasing, work system design, engineering design and production planning. In any case, a benchmarking project, like any project, needs to be carefully scoped with terms of reference and be properly managed. This process is set out in Figure 13.4 [on the following page].
Many organisations confuse ‘benchmarking’ with simply ‘comparing yourself with another organisation’. While this may be helpful, benchmarking means actively seeking out the best and learning from them.
A key stage, then, is the selection of a benchmarking partner, usually found through network or identified by external parties such as consultants, industry associations or insurers. For an organisation to become a benchmarking partner, they must be willing to share their experience at some cost to their time and resources. This often rules out direct industry competitors who fear ‘spies’. The benefits for a benchmarking partner are seeing any effort to reduce workplace injuries as worthwhile and the opportunity to show off their leadership and brand. Benchmarking partners needn’t come from the same industry and often the most interesting lessons can come from ‘best practitioners’ in different areas of the economy; it depends on the areas being benchmarked.
Other conditions for successful benchmarking by both partners include:
- a commitment, particularly from senior management to WHS benchmarking (time, resources)
- a commitment to a preventive and systematic approach to WHS
- use of consultation.
Teams
Teams allow a range of expertise, experience and representation to be involved. Benchmarking teams should:
- involve management and employee representatives with the required expertise in the areas being benchmarked
- be limited to six at the maximum
- receive training in the required skills and knowledge.
An important by-product of benchmarking is the training and experience acquired by those involved. While it can be tricky and resource-consuming, benchmarking can be very beneficial and not just for HS performance.
| Step 1 | Establish benchmarking project |
|---|---|
| Step 2 | Select teams and train them |
| Step 3 | Identify processes to benchmark |
| Step 4 | Analyse your own processes |
| Step 5 | Select benchmarking partners |
| Step 6 | Build relationships and conduct visits |
| Step 7 | Analyse performance gaps and develop improvement strategies |