
Readings in sections of the learning are associated with the units:
- Work with diverse people (CHCDIV001)
- Promote Aboriginal and/or Torres Strait Islander Cultural Safety (CHCDIV002)
Readings
- Reading A: Understanding and Applying Intercultural Communication in the Global Community
- Reading B: Cultural Diversity in Australia
- Reading C: Working with People from Culturally and Linguistically Diverse Backgrounds
- Reading D: Communicating Effectively with Aboriginal and Torres Strait Islander People
- Reading E: Why Cultural Safety Rather than Cultural Competency
- Reading F: White Privilege: Unpacking the Invisible Knapsack
- Reading G: Welcome to Country & Acknowledgement of Country
- Reading H: Working with Indigenous Children, Families, and Communities: Lessons from Practice
- Reading I: Creating Change Through Partnerships
- Reading J: Participatory Evaluation
All Case Histories in this text are presented as examples only and any comparison which might be made with persons either living or dead is purely coincidental.

McDaniel, E. R., & Samovar, L. A. (2015). Understanding and Applying Intercultural Communication in the Global Community: The Fundamentals. In L. A. Samovar, R. E., Porter, E. R., McDaniel, & C. S. Roy (Eds.) In Intercultural Communication: A Reader (14th ed.) (pp. 10-16).
What Culture Does
If we accept the idea that culture can be viewed as a set of social rules, its purpose becomes self-evident. Cultural rules provide a framework that gives meaning to events, objects, and people. The rules enable us to make sense of our surroundings and reduce uncertainty about the social environment. Recall the first time you were introduced to someone you were attracted to. You probably felt some level of nervousness because you wanted to make a positive impression. During the interaction you may have had a few thoughts about what to do and what not to do. Overall, you had a good idea of the proper courtesies, what to talk about, and generally how to behave. This is because you had learned the proper cultural rules of behavior by listening to and observing others. Now, take that same situation and imagine being introduced to a student from a different country, such as Jordan or Kenya. Would you know what to say and do? Would the cultural rules you had been learning since childhood be effective, or even appropriate, in this new social situation?
Culture also provides us with our identity, or sense of self. From childhood, we are inculcated with the idea of belonging to a variety of groups – family, community, church, sports teams, schools, and ethnicity – and these memberships form some of our different identities. Our cultural identity is derived from our “sense of belonging to a particular cultural or ethnic group” (Lustig & Koester, 2006, p. 3), which may be Chinese, Mexican American, African American, Greek, Egyptian, Jewish, or one or more of many, many other possibilities. Growing up, we learn the rules of social conduct appropriate to our specific cultural group, or groups in the case of multicultural families such as Vietnamese American, Italian American, or Russian American. Cultural identity can become especially prominent during interactions between people from different cultural groups, such as Pakistani Muslim and an Indian Hindu, who have been taught varied values, beliefs, and different sets of rules for social interaction. Thus, cultural identity can be a significant factor in the practice of intercultural communication.
Culture’s Components
While there are many explanations of what culture is and does, there is general agreement on what constitutes its major characteristics. An examination of these characteristics will provide increased understanding of this abstract, multifaceted concept and also offer insight into how communication is influenced by culture.
Culture is Learned
At birth, we have no knowledge of the many societal rules needed to function effectively in our culture, but we quickly begin to internalize this information. Through interactions, observations, and imitation, the proper ways of thinking, feeling, and behaving are communicated to us. Being taught to eat with a fork, a pair of chopsticks, or even one’s fingers is learning cultural behavior. Attending a Catholic mass on Sunday or praying at a Jewish Synagogue on Saturday is learning cultural behaviors and values. Celebrating Christmas, Kwanza, Ramadan, Yom Kippur is learning cultural traditions. Culture is also acquired from art, proverbs, folklore, history, religion, and a variety of other sources. This learning, often referred to an enculturation, is both conscious and subconscious and has the objective of teaching the individual how to function properly within a specific cultural environment.
Culture is Transmitted Intergenerationally
Spanish philosopher George Santayana wrote, “Those who cannot remember the past are condemned to repeat it.” He was certainly not referring to culture, which exists only if it is remembered and repeated by people. You learned your culture from family members, teachers, peers, books, personal observations, and a host of media sources. The appropriate way to act, what to say, and things to value were all communicated to the members of your generation by these many sources. You are also a source for passing these cultural expectations to succeeding generations, usually with little or no variation. Culture represents our link to the past and, through future generations, hope for the future. The critical factor in this equation is communication.
Culture Is Symbolic
Words, gestures, and images are merely symbols used to convey meaning. It is the ability to use these symbols that allows us to engage in the many forms of social intercourse used to construct and convey culture. Our symbol-making ability facilitates learning and enables transmission of meaning from one person to another, group to group, and generation to generation. In addition to transmission, the portability of symbols creates the ability to store information, which allows cultures to preserve what is considered important, and to create a history. The preservation of culture provides each new generation with a road map to follow and a reference library to consult when unknown situations are encountered. Succeeding generations may modify established behaviors or values, or construct new ones, but the accumulation of past traditions is what we know as culture.
Culture Is Dynamic
Despite its historical nature, culture is never static. Within a culture, new ideas, inventions, and exposure to other cultures create change. Discoveries such as the stirrup, gunpowder, the nautical compass, penicillin, and nuclear power are examples of culture’s susceptibility to innovation and new ideas. More recently, advances made by minority groups, the women’s movement, and gay rights advocates have significantly altered the fabric of contemporary U.S. society. Invention of the computer chip, the Internet, and the discovery of DNA have brought profound changes not only to U.S. culture but also to the rest of the world.
Diffusion, or cultural borrowing, is also a source of change. Think about how common pizza (Italian), sushi (Japanese), tacos (Mexican), and tandoori chicken and naan bread (India) are to the U.S. American diet. The Internet has accelerated cultural diffusion by making new knowledge and insights easily accessible. Immigrants bring their own cultural practices, traditions, and artifacts, some of which become incorporated into the culture of their new homeland, for example, Vietnamese noodle shops in the United States, Indian restaurants in England, or Japanese foods in Brazil.
Cultural calamity, such as war, political upheaval, or large-scale natural disasters, can cause change. U.S. intervention in Afghanistan is bringing greater equality to the women of that nation. For better or worse, the invasion of Iraq raised the influence of Shia and Kurdish cultural practices and lessened those of the Sunni. International emergency relief workers responding to the earthquake and tsunami disaster in Japan brought their own cultural practices to the situation, some of which no doubt became intermingled with the cultural practices of the local Japanese.
Immigration is a major source of cultural discussion. Many of the large U.S. urban centers now have areas unofficially, called Little Italy, Little Saigon, Little Tokyo, Korea Town, China Town, Little India, etc. These areas are usually home to restaurants, markets, and stores catering to a specific ethnic group. However, they also serve to introduce different cultural practices to other segments of the population.
Most of the changes, are often topical in nature, such as dress, food preference, modes of transportation, or housing. Values, ethics, morals, the importance of religion, or attitudes toward gender, age, and sexual orientation, which constitute the deep structures of culture, are far more resistant to major change and tend to endure from generation to generation.
Culture Is Ethnocentric
The strong sense of group identity, or attachment, produced by culture can also lead to ethnocentrism, the tendency to view one’s own culture as superior to others. Ethnocentrism can arise from enculturation. Being continually told that you live in the greatest country in the world or that the United States is “exceptional,” or that your way of life is better than those of other nations, or that your values are superior to those of other ethnic groups can lead to feelings of cultural superiority, especially among children. Ethnocentrism can also result from a lack of contact with other cultures. If exposed only to a U.S. cultural orientation, it is likely that you would develop the idea that your way of life was superior, and you would tend to view the rest of the world from that perspective.
An ability to understand or accept different ways and customs can also provoke feelings of ethnocentrism. It is quite natural to feel at ease with people who are like you and adhere to the same social norms and protocols. You know what to expect, and it is usually easy to communicate. It is also normal to feel uneasy when confronted with new and different social values, beliefs, and behaviors. You do not know what to expect, and communication is probably difficult. However, to view or evaluate those differences negatively simply because they vary from your expectations is a product of ethnocentrism, and an ethnocentric disposition is detrimental to effective intercultural communication.
Integrating Communication and Culture
There are a number of culture related components important in the study of intercultural communication. These include (1) perception, (2) patterns of cognition, (3) verbal behaviors, (4) nonverbal behaviors, and (5) the influence of context. Although each of these components will be discussed separately you must keep in mind that in an intercultural setting, all become integrated and function at the same time.
Perception
Every day we encounter an overwhelming amount of varied stimuli that we must cognitively process and assign a meaning. This procedure of selecting, organizing and evaluating stimuli is referred to as perception. The volume of environmental stimuli is far too large for us to pay attention to everything, so we select only what is considered relevant or interesting. After determining what we will attend to, the next step is to organize the selected stimuli for evaluation. Just as in this book, the university library, media news outlets, or Internet web sites, information must be given a structure before it can be interpreted. The third step of perception then involves evaluating and assigning meaning to the stimuli.
A common assumption is that people conduct their lives in accordance with how they perceive the world, and these perceptions are strongly influenced by culture. In other words, we see, hear, feel, taste, and even smell the world through the criteria that culture has placed on our perceptions. Thus, one’s idea of beauty, attitude toward the elderly, concept of self in relation to others, and even what tastes good and bad are culturally influenced and can vary among social groups. For example, Vegemite is a yeast extract spread used on toast and sandwiches that is sometimes referred to as the “national food” of Australia. Yet, few people other than those from Australia or New Zealand like the taste, or even the smell, of this salty, dark paste spread.
As you would expect, perception is a critical aspect of intercultural communication, because people from dissimilar cultures frequently perceive the world differently. Thus, it is important to be aware of the relevant socio-cultural elements that have a significant and direct influence on the meanings we assign to stimuli. These elements represent our belief, value, and attitude systems and our worldview.
Beliefs, Values, and Attitudes
Beliefs
can be defined as individually held subjective ideas about the nature of an object or event. These subjective ideas are, in large part, a product of culture, and they directly influence our behaviors. Bull fighting is generally thought to be cruel and inhumane by most people in the United States but many people in the Spain and Mexico consider it part of their cultural heritage. Strict adherents of Judaism and Islam believe eating pork is forbidden, but in China, pork is staple. In religion, many people believe there is only one god but others pay homage to multiple deities.
Values
Represent those things we hold important in life, such are morality, ethics, and aesthetics. We use values to distinguish between the desirable and the undesirable. Each person has a set of unique personal values and a set of cultural values. The latter are a reflection of the rules a culture has established to reduce uncertainty, lessen the likelihood of conflict, help in decision making, and provide structure to social organization and interactions. Cultural values are a motivating force behind our behaviors. Someone from a culture that places a high value on harmonious social relations, such as Korea and Japan, will likely employ an indirect communication style. In contrast, a U.S. American can be expected to use a more direct style because frankness, honesty, and openness are valued.
Attitudes
Our beliefs and values push us to hold certain attitudes, which are learned tendencies to act or respond in a specific way to events, objects, people, or orientations. Because culturally instilled beliefs and values exert a strong influence on attitudes, people tend to embrace what is liked and avoid what is disliked. Someone from a culture that considers cows sacred will surely take a negative attitude toward your invitation to have an Arby’s roast beef sandwich for lunch.
Worldview
Although quite abstract, the concept of worldview is among the most important elements of the perceptual attributes influencing intercultural communication. Stated simply, worldview is what forms an individual’s orientation toward such philosophical concepts as God, the universe, nature, and the like. Normally, worldview is deeply imbedded in one’s psyche and usually operates on a subconscious level. This can be problematic in an intercultural situation, where conflicting worldviews can come into play. As an example, many Asian and Native North American cultures hold a worldview that people should have a harmonious, symbiotic relationship with nature. In contrast, Euro-Americans are instilled with the concept that people must conquer and mold nature to conform to personal needs and desires. Individuals from nations possessing these two contrasting worldviews could well encounter difficulties when working to develop an international environmental protection plan. The concept of democracy, with everyone having an equal voice in government, is an integral part of the U.S. worldview. Contrast this with Afghanistan and parts of Africa where the worldview holds that one’s tribe or clan takes precedence over the central government.
Cognitive Patterns
Another important consideration in intercultural communication is the influence of culture on cognitive thinking patterns, which include reasoning and approaches to problem solving. Culture often produces different ways of knowing and doing. Research by Nisbett (2003) has demonstrated that Westerners use a linear, cause-and-effect thinking process, which places considerable value on logical reasoning and rationality. Thus, problems can be best solved by a systematic, in-depth analysis of each component, progressing individually from the simple to the more difficult. In contrast, Nisbett’s research disclosed that Northeast Asians (Chinese, Japanese, and Koreans) employ a holistic thinking pattern. They see problems as much more complex and interrelated, requiring a greater understanding of, and emphasis on, the collective rather than focusing separately on individual parts.
A culture’s normative thought patterns will influence the way individuals communicate and interact with each other. However, what is common in one culture may be problematic in another culture. As an illustration, in Japanese-U.S. business negotiations, the Japanese have a tendency to reopen previously discussed issues that the U.S. side considers resolved. United States negotiators find this practice to be frustrating and time consuming, believing that once a point has been agreed upon, it is completed. From the Japanese holistic perspective, however, new topics can have an influence on previously discussed points (McDaniel, 2000). This example demonstrates the importance of understanding that variant patterns of cognition exist and the need to learn how to accommodate them in an intercultural communication encounter.
Nonverbal Behavior
Another critical factor in intercultural communication is nonverbal behavior, which includes gestures, facial expressions, eye contact and gaze, posture and movement, touch, dress, silence, the use of space and time, objects and artifacts, and paralanguage. These nonverbal activities are inextricably intertwined with verbal behaviors and often carry as much or more meaning than the actual spoken words. As with language, culture also directly influences the use of, and meanings assigned to, nonverbal behavior. In intercultural communication, inappropriate or misused nonverbal behaviors can easily lead to misunderstandings and sometimes result in insults. A comprehensive examination of all nonverbal behavior is beyond the scope of this chapter, but we will draw on a few culturespecific examples to demonstrate their importance in intercultural communication exchanges.
Nonverbal greeting behaviors show remarkable variance across cultures. In the United States, a firm handshake among men is the norm, but in some Middle Eastern cultures, a gentle grip is used. In Mexico, acquaintances will often embrace (abrazo) each other after shaking hands. Longtime Russian male friends may engage in a bear hug and kiss each other on both cheeks. People from Japan and India traditionally bow to greet each other. Japanese men will place their hands at the side of the body and bow from the waist, with the lower-ranking person bowing first and dipping lower that the other person. Indians will perform the namaste, which entails holding the hands together in a prayer-like fashion at mid-chest while slightly bowing the head and shoulders.
Eye contact is another important culturally influenced nonverbal communication behavior. For U.S. Americans, direct eye contact is an important part of making a good impression during an interview. However, in some cultures, direct eye contact is considered rude or threatening. Among some Native Americans, children are taught to show adults respect by avoiding eye contact. When giving a presentation in Japan, it is common to see people in the audience with their eyes shut, because this is thought to facilitate listening. (Try it – you may be surprised.) How a person dresses also sends a strong nonverbal message. What are your thoughts when you see an elderly woman wearing a hijab, a Jewish boy with yarmulke, or a young black man in a colourful dashiki?
Nonverbal facial and body expressions, like language, form a coding system for constructing and expressing meaning, and these expressions are culture bound. Through culture, we learn which nonverbal behavior is proper for different social interactions. But what is appropriate and polite in one culture may be disrespectful or even insulting in another culture. People engaging in intercultural communication, therefore, should try to maintain a continual awareness of how body behaviors may influence an interaction.
Contextual Influences
We have defined culture as a set of rules established and used by a group of people to conduct social interactions. These rules determine what is considered correct communicative behavior, including both verbal and nonverbal elements, for both physical and social (situational) contexts. For example, you would not normally attend a funeral wearing shorts and tennis shoes or talk on your cell phone during the service. Your culture has taught you that these behaviors are contextually inappropriate (i.e., disrespectful).
Context is also an important consideration in intercultural communication interactions, where the rules for specific situations usually vary. What is appropriate in one culture is not necessarily correct in another. As an example, among most White U.S. Americans, church services are relatively serious occasions, but among African American congregations, services are traditionally more demonstrative, energetic gatherings. In a restaurant in Germany, the atmosphere is usually somewhat subdued, with customers engaging in quiet conversation. In Spain, however, the conversation is much louder and more animated. In U.S. universities, students are expected to interactively engage the instructor, but in Japan the expectation is that the instructor will simply lecture, with very little or no interaction.
In these examples, we see the importance of having an awareness of the cultural rules governing the context of an intercultural communication exchange. Unless all parties in the exchange are sensitive to how culture affects the contextual aspects of communication, difficulties will most certainly arise and could negate effective interaction.

Australian Bureau of Statistics. (2017). Cultural diversity in Australia: 2016 Census data summary
What is Cultural Diversity?
Cultural diversity relates to a person’s country of birth, their ancestry, the country of birth of their parents, what languages they speak, whether they are of Aboriginal or Torres Strait Islander descent, and their religious affiliation. The Census collects information on many characteristics that highlight the rich cultural diversity of Australian society.
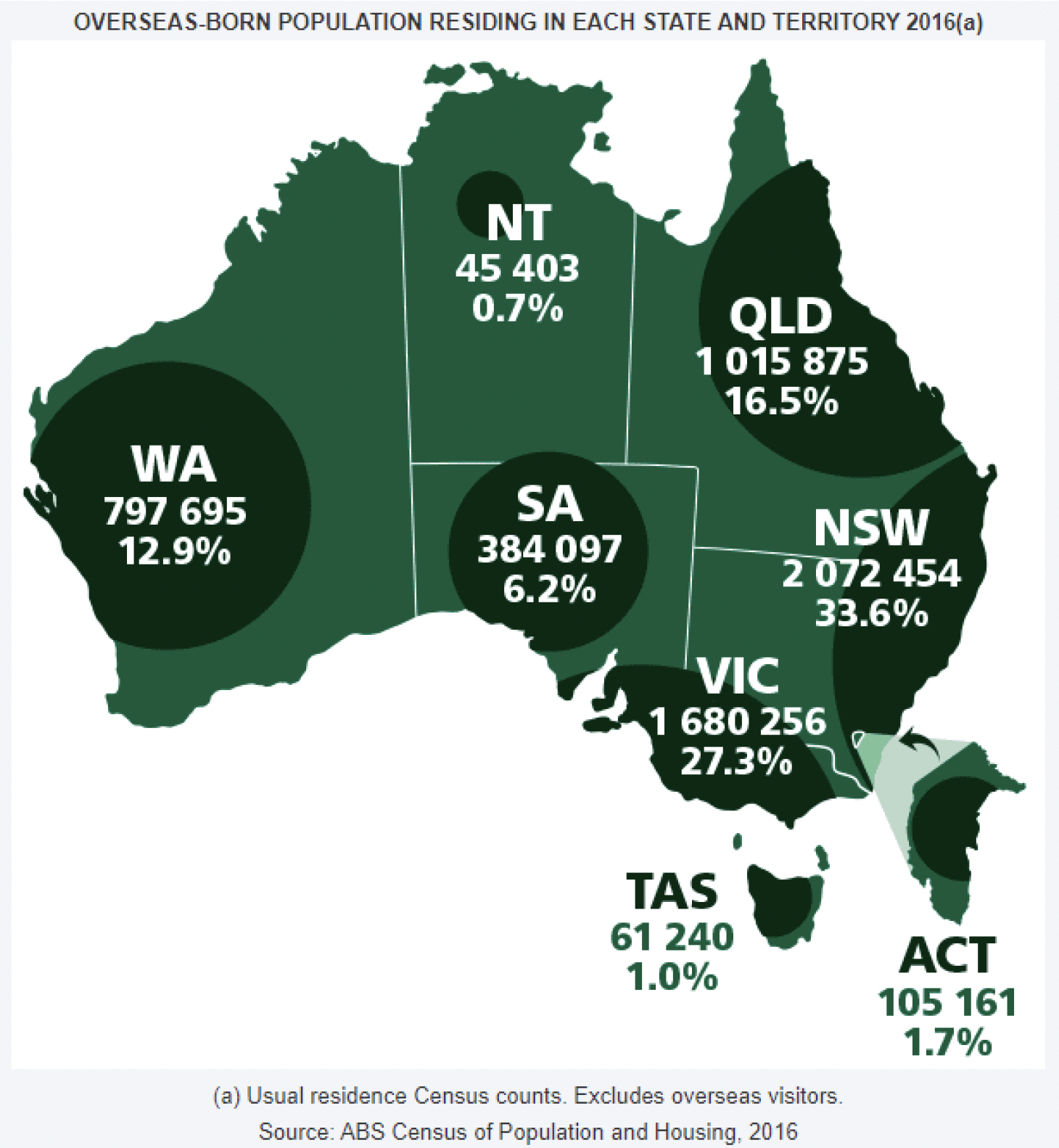
Country of Birth
The 2016 Census shows that two thirds (67%) of the Australian population were born in Australia. Of the 6,163,667 overseas-born persons, nearly one in five (18%) had arrived since the start of 2012.
While England and New Zealand were still the next most common countries of birth after Australia, the proportion of those born overseas who were born in China and India has increased since 2011 (from 6.0% to 8.3%, and 5.6% to 7.4% respectively).
The Philippines has swapped places with Italy in the top 10 list, moving from number 8 to number 6.
Malaysia now appears in the top 10 countries of birth (replacing Scotland) and represents 0.6% of the Australian population.
| Top Five | 2011 | 2016 | |
|---|---|---|---|
| Country | % | ||
| 1 | Australia | 68.8 | 66.7 |
| 2 | England | 4.2 | 3.9 |
| 3 | New Zealand | 2.2 | 2.2 |
| 4 | China | 1.5 | 2.2 |
| 5 | India | 1.4 | 1.9 |
Ancestry
Ancestry is an indication of the cultural group that a person most closely identifies with.
Over 300 ancestries were separately identified in the 2016 Census. The most commonly reported ancestries were English (36%) and Australian (34%).
A further six of the leading ten ancestries reflected a European heritage. The two remaining ancestries in the top 10 were Chinese (5.6%) and Indian (4.6%).

Languages
In 2016, there were over 300 separately identified languages spoken in Australian homes. More than one-fifth (21%) of Australians spoke a language other than English at home.

Aboriginal and Torres Strait Islander Peoples
649 171 - 2.8% of the Australian population
The Aboriginal and Torres Strait Islander population has increased since 2011 from 2.5% to 2.8% of the Australian population. Further information on the Aboriginal and Torres Strait Islander population is available in the Aboriginal and Torres Strait Islander Population data summary.
Religion
| Religous Affiliations Reported by the Australian Population, 2016 | |||
|---|---|---|---|
| Religous | Population ('000) | Population (%) | |
| Christian | 12 201.6 | 52.1 | |
| Other Religions | Islam | 604.2 | 2.6 |
| Buddhism | 563.7 | 2.4 | |
| Hinduism | 440.3 | 1.9 | |
| Sikhism | 125.9 | 0.5 | |
| Judaism | 91.0 | 0.4 | |
| Other | 95.7 | 0.4 | |
| Total | 1 920.8 | 8.2 | |
| No Religion a | 7 040.7 | 30.1 | |
| Australia b | 23 401.9 | 100.0 | |
a = No religion includes secular and other spiritual beliefs.
b = As religion was an optional question, the total for Australia will not equal the sum of the items above it.
In 2016, Christianity was the main religion reported in Australia (52%).
While the Islamic population made up only 2.6% of the total population, it was the second largest religion reported in the 2016 Census after Christianity. Islam was closely followed by Buddhism (2.4%).
The 'No Religion' count increased to almost a third of the Australian population between 2011 and 2016 (22% to 30%).
The Generations of Australians
In 2016, nearly half (49%) of Australians had either been born overseas (first generation Australian) or one or both parents had been born overseas (second generation Australian).

Where Migrants Live
For Australia's overseas-born population, New South Wales was still the most popular state or territory to live in 2016 (2,072,454 people or 34% of the overseas-born population).

Queensland Government (2010). Working with people from culturally and linguistically diverse backgrounds. (pp. 17-23).
There are no recipes or blueprints for working with people from specific cultural backgrounds (Diversity Training Manual, Immigrant Women’s Support Service, 2002: 120).
It is neither feasible nor appropriate to provide a prescriptive approach for working with people from specific ethnic, cultural or linguistic backgrounds. However based on the information and issues previously outlined in this paper, a number of effective approaches to practice are available for implementation by departmental officers, when intervening with children and families from culturally and linguistically diverse backgrounds.
Use appropriate terminology and avoid stereotyping
It is critical for staff working with children and families from a culture or ethnic group different from their own to recognise the uniqueness of all people and avoid stereotyping or making assumptions based on a person’s ethnicity, religion, culture or language. It is also important to be aware of the potential sensitivities around the use of some terminology.
Using terms such as “culturally and linguistically diverse”, “non-English speaking”, or “migrant” when referring to someone could be offensive as it may be taken to imply that the person is being categorised or is not part of the broader Australian community. For example, while it may be accurate to describe someone who has recently settled in Australia as a “migrant”, this would not be appropriate after a certain period of time unless the person chooses to self-identify in that way.
Develop cross-cultural competence
It would be wonderful if, with the wave of a magic wand, we could all possess the skills and attitudes that it takes to be cross-culturally effective. But, unfortunately, there are no shortcuts and there is no magic wand. Acquiring the skills is a lifelong process (Developing Cross-Cultural Competence, A Guide for Working with Children and Their Families, Lynch and Hanson, 2004: 73).
The term “cultural competence” is increasingly being used in relation to working effectively with people from culturally and linguistically diverse backgrounds. There are a number of different definitions provided for the term which typically include reference to organisational systems, policy and practice, as well as to individual workers.
The Standards for Cultural Competence in Social Work Practice published by the National Association of Social Workers (USA) state that:
“Cultural competence refers to the process by which individuals and systems respond respectfully and effectively to people of all cultures, languages, classes, race, ethnic backgrounds, religions, and other diversity factors in a manner that recognises, affirms, and values the worth of individuals, families, and communities and protects and preserves the dignity of each”.
While acknowledging both the individual and systemic/organisational context, this section focuses on the development of cultural competence at the individual level. Cultural competence at a personal level encompasses the worker’s attitudes, knowledge and skills, and requires an acceptance that long-term, ongoing and persistent development is required.
There are three key elements that are commonly identified in the development of cultural competence. These are:
- Developing cultural awareness, including self-awareness about one’s own culture
- Acquiring knowledge about other cultures
- Developing cross-cultural skills
Developing cultural awareness, including self-awareness
About one’s own culture, and associated values and assumptions on behaviour and interactions, is the first step towards developing cultural competence (Lynch and Hanson, 2004). This can often be difficult for people who belong to the dominant Anglo-Australian culture, as “culture” and “cultural diversity” are typically seen as pertaining to “others”. This process includes acknowledging any personal biases and stereotypes, recognising the influence of cultural norms and attitudes, and valuing cultural diversity and the validity of differing beliefs and values.
Acquiring knowledge about other cultures
Is another key element to developing cultural competence, and may be achieved by interacting with people from other cultural backgrounds in both professional and personal life, talking with service providers and community organisations who work with culturally diverse people, researching, watching films or documentaries or reading about other cultures and cultural diversity, and participating in workshops and seminars.
It is unrealistic to expect departmental officers to gain a thorough understanding about every cultural and ethnic group within Queensland. However, identifying the various cultural and ethnic communities that live in the area where you work and developing some understanding about their cultures is a useful starting point.
Developing cross-cultural skills
The third key element of cultural competency, includes:
- Effective cross-cultural communication
- Working with interpreters and translators
- Developing collaborative models with ethno-specific agencies and those working with people from culturally and linguistically diverse backgrounds
- Establishing effective relationships with people from culturally and linguistically diverse backgrounds
- Reflecting on and learning from each interaction with people from different cultures to inform future practice
- Monitoring access to services by people from culturally and linguistically diverse backgrounds through data collection
- Identifying practices and systems that hinder cultural competency
- Identifying and implementing approaches that remove any barriers to working effectively with people from culturally and linguistically diverse backgrounds.
As with the development of cultural knowledge, there are many ways in which these skills can be acquired. The development of cultural competence needs to be seen as an ongoing process, and every interaction with people from different cultures should be viewed as a learning experience.
Collect and record accurate information about cultural, linguistic and religious identity
How people identify themselves is a key to their self-image. For instance, a person born in Australia to Chinese parents may identify as Chinese, as Chinese Australian, or as Australian. It can lead to misunderstandings if practitioners assume rather than ask individuals how they identify themselves, and about the impact and influence of their cultural background on their life (from Diversity Training Manual, Immigrant Women’s Support Service, 2002: 118).
The identification and collection of accurate and complete information about the cultural, linguistic and religious backgrounds of children and families is critical to ensuring that the needs of the child can be appropriately met, as well as providing an important resource for service planning and for identifying any possible gaps in terms of access to child protection and family support services by parts of the community.
There are a number of provisions in the Child Protection Act 1999 about the need to take account of the ethnic, religious and cultural identity or values of the child. The timely collection of information is a prerequisite to ensuring that these provisions are met.
It is important not to make assumptions about a person’s cultural, linguistic or religious background and not to assume that a person’s country of birth is a reliable indicator of cultural identity. Give each individual the opportunity to self-identify this information by asking them to do so. If the person is unable to provide this information, for example due to a child’s young age, obtain the information from another reliable source, such as a parent.
At the same time, officers should be aware of potential difficulties that they may encounter when trying to collect this information. For example, some people may for various reasons be sensitive or suspicious about the purpose for collecting this information.
These cultural, linguistic and religious sensitivities may be able to be allayed by explaining that the information is being sought to ensure that the needs of the child and the child’s family can be appropriately responded to. Giving assurances about the department’s privacy and confidentiality policies may also assist.
The nature of information to be collected and recorded by departmental officers, when intervening with people from CALD backgrounds, is outlined in the Department of Communities, Child Safety Policy No. 458-2, Cultural Diversity Data Collection and Reporting.
Develop effective cross-cultural communication skills
Communication, both verbal and nonverbal, is critical to cross-cultural competence. Both sending messages and understanding messages that are received are pre-requisites to effective interpersonal interactions. Because language and culture are so inextricably bound, communicating with families from different cultural and/or sociocultural backgrounds is very complex (from Developing Cross-Cultural Competence, A Guide for Working with Children and Their Families, Lynch and Hanson, 2004: 61).
An understanding of some general principles and guidelines for effective cross-cultural communication can assist staff to be more effective when communicating with children and families from a cultural background different from their own. Lynch and Hanson (2004: 34) identify the importance of understanding that there are cultural differences in non-verbal communication, and of acknowledging cultural differences rather than minimising them in relation to cross-cultural communication.
Non-verbal communication can vary significantly across different cultures, and may sometimes even have an opposite meaning. For example, maintaining eye contact is valued during interpersonal interactions in most Anglo-based cultures, and is seen as conveying trustworthiness and sincerity. However, in a number of cultures, making eye contact with someone in authority is seen as a sign of disrespect, and in some cultures eye contact between strangers may be considered shameful. Similarly, smiling or laughing in some cultures may be used when describing an event that is confusing, embarrassing or even sad.
There are also cultural differences relating to physical proximity and social distance; touching and other physical contact; physical postures and gestures. Nodding a head is generally taken as a sign of understanding or agreement in mainstream Anglo-based cultures, however in some other cultures it may only signal an acknowledgment that you are speaking without implying either understanding or agreement. While it is not reasonable to expect anyone to know the range of non-verbal communication patterns across cultures, it is important to be aware of the potential for misunderstanding in these areas.
In some cultures there is a strong imperative to avoiding a display of disagreement and conflict. Individuals may appear to agree to a plan of action to avoid what they experience as an embarrassing or challenging situation, with no real capacity or intention to comply with the plan.
Acknowledging and respecting cultural differences rather than minimising them is important for effective cross-cultural communication, with the following characteristics being identified as common to effective cross-cultural communicators (Lynch and Hanson 2004):
- Having respect for people from other cultures
- Making continued and sincere attempts to understand the world from others’ points of view
- Being open to new learning
- Being flexible
- Having a sense of humour
- Tolerating ambiguity well
- Approaching others with a desire to learn.
Some other practical guidelines include:
- Use an accredited professional interpreter when a person is unable to communicate effectively in English (see below)
- Check and use correct pronunciation of names and the correct or preferred way of addressing a person (for example, formally or informally)
- Use plain English and clear enunciation
- Use concrete instead of abstract language and avoid the use of idioms, irony, sarcasm, slang and jargon
- Be patient, receptive and listen carefully to everything that is said
- Avoid any tendency to equate the person’s level of language skill or accent with level of intelligence or credibility
- Ask open-ended questions and be aware that the repeated “yes” answers may mean different things in different cultural contexts
- Make sure that the other person understands what you have said and that you understand what they have said. This can be done by asking the person to tell you what they have understood you have said and by paraphrasing back to them what you understand they have said.
Finally, it is useful to reflect on each cross-cultural interaction to identify those things that went well and areas that could be improved.
Utilise interpreters
The Queensland Government recognises that a significant number of people do not speak English at all or well enough to communicate adequately with officers of Queensland Government agencies… agencies should provide an interpreter in situations where a non-English speaking client has difficulty communicating in English (from Queensland Government Language Services Policy, 2004: 8).
Interpreters should be engaged in any situation where a child or family member has difficulty communicating in English. Wherever possible, a professional, qualified interpreter who has been accredited by the National Accreditation Authority for Translators and Interpreters (NAATI) should be used. They operate under a code of ethics and have been trained in areas such as maintaining confidentiality and accuracy.
As noted previously, children sometimes become proficient in English more quickly than their parents. However, as noted in the Queensland Government Language Services Policy, “Children and young relatives are not appropriate interpreters in any context.” (from Queensland Government Language Services Policy, 2004: 10). Similarly, the use of other family members or friends of the family as interpreters is also problematic and needs to be avoided. Some of the problems with using family members or friends as interpreters include the potential for embarrassment for all parties, and the increased risk of miscommunication and lack of privacy.
The need for an interpreter may not always be obvious, as some people may be able to converse at a basic level in English but not necessarily fully understand the language used by professionals. If there is any doubt about the person’s ability to fully comprehend what is being communicated, an interpreter should be used.
When engaging an interpreter it is important to confirm the language and dialect needs of the client, any gender preferences that they might have in relation to the interpreter and the preferred interpreting mode. Interpreting services may be available both on-site and through telephone interpreting.
Telephone interpreting has the benefits of being more readily available in regional areas and offering access to interpreters in a greater range of languages through a national network. On the other hand, on-site interpreting has the benefit of allowing for visual and non-verbal cues which can facilitate the communication, as well as the possibility of continuity as the same interpreter can be requested and used.
Another critical consideration when engaging an interpreter is to check that the interpreter is acceptable to the child and parents. In some circumstances, especially in smaller or emerging communities in which there are a limited number of accredited interpreters, the interpreter may be known to the child or family which could significantly inhibit or otherwise compromise the interaction.
Some suggested guidelines for staff when working with interpreters that are referred to in the literature include:
- Brief the interpreter beforehand wherever possible, explaining the purpose of the interview or meeting
- Allow for the extra time that is likely to be needed when using an interpreter
- Introduce yourself and the interpreter to the client and explain clearly who you are and what your role is
- Speak directly to the client rather than addressing the client through the interpreter and look at the client when speaking and listening to them
- Maintain control of the interview
- Pause often to allow the interpreter to speak
- Speak clearly and somewhat more slowly but not loudly
- Avoid using slang or technical jargon
- Make sure that the interpreter understands any difficult concepts that you are trying to convey
- Periodically check on the client’s understanding of what has been said by asking them, through the interpreter, to repeat in their own words what has been communicated
- Summarise what has been agreed during the meeting and check if the client has any questions
- Debrief the interpreter if necessary after the interview once the client has left.
Information about translating and interpreting services is available through the Multicultural Affairs Queensland website.
Establish links with service providers and ethnic community organisations
The insufficient partnership between the child safety services, community service providers in child safety and CALD communities was highlighted as a barrier to a better understanding of child safety legislation (from Changing the Wheels: Child Safety Concerns in Queensland, 2005:23).
There are a number of ethnic community organisations and service providers with strong links to people from culturally and linguistically diverse backgrounds throughout Queensland. Establishing links with these services can assist departmental staff to develop their knowledge about working with diversity, as well as the particular needs of children and families. Establishing such links could lead to useful opportunities for working collaboratively to support children at risk and families, and facilitate appropriate referrals to relevant services. Bicultural support workers who can assist both families and departmental staff in their interactions may also be available.
When responding to specific child protection cases, ensure that the child and family’s privacy are protected and that informed consent is given for the involvement of an ethnic community organisation or service provider in each case.
For information about ethnic community organisations and service providers, refer to the Queensland Multicultural Resource Directory, available through the Multicultural Affairs Queensland website.

Queensland Health. (2015). Communicating effectively with Aboriginal and Torres Strait Islander people.
This information sheet provides a general guide for communicating effectively with Aboriginal and Torres Strait Islander people. Further information for communicating in the clinical context can be found in the Aboriginal and Torres Strait Islander Patient Care Guidelines.
Demonstrating Understanding
The negative impacts of racial and economic disadvantage and a series of past government policies, including segregation, displacement and separation of families has contributed to the mistrust held by Aboriginal and Torres Strait Islander people towards government services and systems.
In today's Western dominant society, Aboriginal and Torres Strait Islander people continue to be a marginalised and socially disadvantaged minority group. Compared to other Australians, Aboriginal and Torres Strait Islander people experience significantly varied outcomes related to health, education, employment and housing. Discrimination, racism and lack of cultural understanding mean that Aboriginal and Torres Strait Islander people still experience inequality and social injustice.
People's cultural beliefs, values and world-views influence thinking, behaviours and interactions with others. It is important to reflect without judgement before, during and after interacting with people whose beliefs, values, world-views and experiences are different to your own.
Personal Communication
Rapport
In many traditional cultures, a high sense of value is placed on building and maintaining relationships. Taking a 'person before business' approach will help form this relationship and build rapport.
- Introduce yourself in a warm and friendly way.
- Ask where people are you from, share stories about yourself or find other topics of common interest.
Language
Many Aboriginal and Torres Strait Islander people do not speak English as their first language. Some also speak English in different dialects such as Kriol, Aboriginal English and Torres Strait Creole.
Some general tips to overcome language barriers may include:
- Avoid using complex words and jargon.
- Explain why you need to ask any questions.
- Always check you understood the meaning of words the person has used and vice versa.
- Use diagrams, models, dvds and images to explain concepts, instructions and terms.
- Be cautious about using traditional languages or creole words unless you have excellent understanding.
- If required, seek help from local Aboriginal and Torres Strait Islander staff.
Time
In Western culture, emphasis is placed on time to meet deadlines and schedules. Time is perceived differently in Aboriginal and Torres Strait Islander cultures, as more value is placed on family responsibilities and community relationships.
- Consider allocating flexible consultation times.
- Take the time to explain and do not rush the person.
Non-Verbal Communication
Some non-verbal communication cues (hand gestures, facial expressions etc.) used by Aboriginal and Torres Strait Islander people have different meanings in the Western context. Be mindful that your own non-verbal communication will be observed and interpreted. For example, feelings of annoyance may be reflected by your body language and are likely to be noticed.
Personal Space
Be conscious about the distance to which you are standing near a person. Standing too close to a person that you are unfamiliar with, or of the opposite gender, can make a person feel uncomfortable or threatened.
Touch
Always seek permission and explain to the person reasons why you need to touch them. Establish rapport first to make person feel comfortable.
Silence
In Aboriginal and Torres Strait Islander cultures, extended periods of silence during conversations are considered the ‘norm’ and are valued. Silent pauses are used to listen, show respect or consensus. The positive use of silence should not be misinterpreted as lack of understanding, agreement or urgent concerns. Observe both the silence and body language to gauge when it is appropriate to start speaking. Be respectful and provide the person with adequate time. Seek clarification that what was asked or discussed was understood.
Eye Contact
For Aboriginal and Torres Strait Islander people, avoidance of eye contact is customarily a gesture of respect. In Western society averting gaze can be viewed as being dishonest, rude or showing lack of interest. Some (but not all) Aboriginal and Torres Strait Islander people may therefore be uncomfortable with direct eye contact, especially if unfamiliar. To make direct eye contact can be viewed as being rude, disrespectful or even aggressive. To convey polite respect, the appropriate approach would be to avert or lower your eyes in conversation.
- Observe the other person's body language.
- Follow the other person's lead and modify eye contact accordingly.
- Avoid cross-gender eye contact unless the person initiates it and is comfortable.
Titles
In Aboriginal and Torres Strait Islander cultures, the terms ‘Aunty’ or ‘Uncle’ are used to show respect for someone older than you. This person does not have to be a blood relative or necessarily an Elder.
- Only address people with these titles if approval is given and/or a positive relationship exists.
Shame
‘Shame’ (deeply felt feelings of being ashamed or embarrassed) for Aboriginal and Torres Strait Islander people may result from sharing private or personal information, cultural beliefs and from breaches of confidentiality.
- Take a discrete approach and avoid discussions in open or public spaces.
- Build trust and rapport to help people feel safe and comfortable with you and in their surroundings.
- Ensure confidentiality and consider Men’s and Women’s Business.
Listening
Explaining may take time because of narrative communication style or due to linguistic differences. The person may be struggling to communicate what they are trying to get across.
- Avoid selective hearing and ensure you are ‘actively’ listening.
- Paraphrase by summarising and repeating what the person said. This will help with clarification and signal you have been listening.
- Show empathy, be attentive and avoid continually interrupting or speaking over the person.
Questioning
In Aboriginal and Torres Strait Islander cultures, indirect questioning is the approach most preferred. Direct questioning may lead to misunderstandings, discourage participation and make it difficult to obtain important information, particularly when a person is communicating in non-Standard English.
- Use indirect, 'round about' approaches (e.g. frame a question as a statement then allow time for the answer to be given).
- Clarify if the person understood the meanings of your words or questions and that you understood their answers.
- Avoid compound questions (e.g. "how often do you visit your GP and what are the reasons that you don’t?").
- Use plain words (e.g. say ‘start’ rather than ‘commence’).
- Do not ask the person to continually repeat themselves
- Avoid using hypothetical examples.
‘Yes’
Aboriginal and Torres Strait Islander people have a tendency to agree with the questions even when they do not understand or agree, and may answer questions the way they think others want. People may say "yes" to questions to end the conversation so they can leave, to deal with other priorities, or because they simply feel uncomfortable.
- Take the time to build rapport to make the person feel comfortable.
- Explain at the beginning how long the appointment will take and give the person the opportunity to ask questions.
- If a person repeatedly says ‘yes’ immediately after a question, ask with respect what they understood from the questions and/or to explain reasons for their decision.
Clear instructions
It is critical to provide clear and full explanations so that the person fully understands your instructions. For example, to simply say “take until finished” - this may be misunderstood as “take until you feel better” rather than “take until all the tablets are finished”.
Provide options and ownership
When people are given choices and ownership over managing their health, the likelihood of medical compliance is increased.
- Provide options for care; for example, explain how some medications can be taken orally or by injection.
- Ensure that any options are practical and realistic.
- Do not make promises that you cannot deliver as this may create mistrust.
Making decisions
Due to family kinship structures and relationships, decision-making usually involves input by other family members.
- Check with the person if their decisions requires consultation with family.
- Allow time for information to be clearly understood.
- Be respectful if you are asked to leave the room or the meeting for matters to be discussed in private by the family
Communication assistance and cultural support
Build relationships within the local community and learn suitable and generally accepted words. Your local Aboriginal and Torres Strait Islander staff may be able to assist with cultural knowledge and interpreting information. They may also advise you of the best ways of distributing information through the community.

Curtis, E., Jones, R., Tipene-Leach, D., Walker, C., Loring, B., Paine, S. & Reid, P. (2019). Why cultural safety rather than cultural competency is required to achieve health equity: a literature review and recommended definition. International Journal for Equity in Health, 18(174).
Introduction
Internationally, Indigenous and minoritorised ethnic groups experience inequities in their exposure to the determinants of health, access to and through healthcare and receipt of high quality healthcare [1]. The role of health providers and health systems in creating and maintaining these inequities is increasingly under investigation [2]. As such, the cultural competency and cultural safety of healthcare providers are now key areas of concern and issues around how to define these terms have become paramount, particularly within a Aotearoa New Zealand (NZ) context [3]. This article explores international literature to clarify the concepts of cultural competency and cultural safety in order to better inform both local and international contexts.
In NZ, Māori experience significant inequities in health compared to the non-Indigenous population. In 2010–2012, Māori life expectancy at birth was 7.3 years less than non-Māori [4] and Māori have on average the poorest health status of any ethnic group in NZ [5, 6]. Although Māori experience a high level of health care need, Māori receive less access to, and poorer care throughout, the full spectrum of health care services from preventative to tertiary care [7, 8]. This is reflected in lower levels of investigations, interventions, and medicines prescriptions when adjusted for need [8, 9]. Māori are consistently and significantly less likely to: get understandable answers to important questions asked of health professionals; have health conditions explained in understandable terms; or feel listened to by doctors or nurses [10]. The disturbing health and social context for Māori and significant inequities across multiple health and social indicators described above provide the ‘needs-based’ rationale for addressing Māori health inequities [8]. There are equally important ‘rights-based’ imperatives for addressing Indigenous health and health equity [11], that are reinforced by the United Nations Declaration on the Rights of Indigenous Peoples [12] and Te Tiriti o Waitangi (Treaty of Waitangi) in NZ.
There are multiple and complex factors that drive Indigenous and ethnic health inequities including a violent colonial history that resulted in decimation of the Māori population and the appropriation of Māori wealth and power, which in turn has led to Māori now having differential exposure to the determinants of health [13] [14] and inequities in access to health services and the quality of the care received. Framing ethnic health inequities as being predominantly driven by genetic, cultural or biological differences provides a limited platform for in-depth understanding [15, 16]. In addition, whilst socio-economic deprivation is associated with poorer health outcomes, inequities remain even after adjusting for socio-economic deprivation or position [17]. Health professionals and health care organisations are important contributors to racial and ethnic inequities in health care [2, 13]. The therapeutic relationship between a health provider and a patient is especially vulnerable to the influence of intentional or unintentional bias [18, 19] leading to the “paradox of well-intentioned physicians providing inequitable care [20]. Equitable care is further compromised by poor communication, a lack of partnership via participatory or shared decision-making, a lack of respect, familiarity or affiliation and an overall lack of trust [18]. Healthcare organisations can influence the structure of the healthcare environment to be less likely to facilitate implicit (and explicit) bias for health providers. Importantly, it is not lack of awareness about ‘the culture of other groups’ that is driving health care inequities - inequities are primarily due to unequal power relationships, unfair distribution of the social determinants of health, marginalisation, biases, unexamined privilege, and institutional racism [13]. Health professional education and health institutions therefore need to address these factors through health professional education and training, organisational policies and practices, as well as broader systemic and structural reform.
Eliminating Indigenous and ethnic health inequities requires addressing the social determinants of health inequities including institutional racism, in addition to ensuring a health care system that delivers appropriate and equitable care. There is growing recognition of the importance of cultural competency and cultural safety at both individual health practitioner and organisational levels to achieve equitable health care delivery. Some jurisdictions have included cultural competency in health professional licensing legislation [21], health professional accreditation standards, and pre-service and in-service training programmes [22,23,24,25]. However, there are mixed definitions and understandings of cultural competency and cultural safety, and how best to achieve them. This article reviews how concepts of cultural competency and cultural safety (and related terms such as cultural sensitivity, cultural humility etc) have been interpreted. The unintended consequences of a narrow or limited understanding of cultural competency are discussed, along with recommendations for why broader conceptualisation of these terms is needed to achieve health equity. A move to cultural safety is recommended, with a rationale for why this approach is necessary. We propose a definition for cultural safety and clarify the essential principles of this approach in healthcare organisations and workforce development.
Methods and Positioning
This review was originally conducted to inform the Medical Council of New Zealand, in reviewing and updating its approach to cultural competency requirements for medical practitioners in New Zealand Aotearoa. The review and its recommendations are based on the following methods:
- An international literature review on cultural competency and cultural safety.
- A review of cultural competency legislation, statements and initiatives in NZ, including of the Medical Council of New Zealand (MCNZ).
- Inputs from a national Symposium on Cultural Competence and Māori Health, convened for this purpose by the MCNZ and Te Ohu Rata o Aotearoa – Māori Medical Practitioners Association (Te ORA) [26].
- Consultation with Māori medical practitioners (through Te ORA).
The authors reflect expertise that includes Te ORA membership, membership of the Australasian Leaders in Indigenous Medical Education (LIME) (a network to ensure the quality and effectiveness of teaching and learning of Indigenous health in medical education), medical educationalist expertise and Indigenous medical practitioner and public health medicine expertise across Australia and NZ. This experience has been at the forefront of the development of cultural competency and cultural safety approaches within NZ. The analysis has been informed by the framework of van Ryn and colleagues [27] which frames health provider behaviour within a broader context of societal racism. They note the importance of shifting “the framing of the problem, from ‘the impact of patient race’ to the more accurate ‘impact of racism’….on clinician cognitions, behaviour, and clinical decision making” [27].
This review and analysis has been conducted from an Indigenous research positioning that draws from Kaupapa Māori theoretical and research approaches. Therefore, the positioning used to undertake this work aligns to effective Kaupapa Māori research practice that has been described by Curtis (2016) as: transformative; beneficial to Māori; under Māori control; informed by Māori knowledge; aligned with a structural determinants approach to critique issues of power, privilege and racism and promote social justice; non-victim-blaming and rejecting of cultural-deficit theories; emancipatory and supportive of decolonisation; accepting of diverse Māori realities and rejecting of cultural essentialism; an exemplar of excellence; and free to dream [28].
The literature review searched international journal databases and the grey literature. No year limits were applied to the original searching. Databases searched included: Medline, Psychinfo, Cochrane SR, ERIC, CINAHL, Scopus, Proquest, Google Scholar, EbscoHost and grey literature. Search terms included MeSH terms of cultural competence (key words: cultural safety, cultural awareness, cultural competence, cultural diversity, cultural understanding, knowledge, expertise, skill, responsiveness, respect, transcultural, multicultural, cross-cultur*); education (key words: Educat*, Traini*, Program*, Curricul*, Profession*, Course*, Intervention, Session, Workshop, Skill*, Instruc*, program evaluation); Health Provider (key words: provider, practitioner, health professional, physician, doctor, clinician, primary health care, health personnel, health provider, nurse); Health Services Indigenous (key words: health services Indigenous, ethnic* Minorit*, Indigenous people*, native people). A total of 51 articles were identified via the search above and an additional 8 articles were identified via the authors’ opportunistic searching. A total of 59 articles published between 1989 and 2018 were used to inform this review. Articles reviewed were sourced from the USA, Canada, Australia, NZ, Taiwan and Sweden (Additional file 1 Table S1).
In addition to clarifying concepts of cultural competence and cultural safety, a clearer understanding is required of how best to train and monitor for cultural safety within health workforce contexts. An assessment of the availability and effectiveness of tools and strategies to enhance cultural safety is beyond the scope of this review, but is the subject of a subsequent review in process.
Reviewing Cultural Competency
Cultural competency is a broad concept that has various definitions drawing from multiple frameworks. Overall, this concept has varying interpretations within and between countries (see Table 1 for specific examples). Introduced in the 1980s, cultural competency has been described as a recognised approach to improving the provision of healthcare to ethnic minority groups with the aim of reducing ethnic health disparities [31].
Table 1 Definitions and Concepts of Related Terms
| Terms | Definition/ Concept Examples | Sources |
|---|---|---|
| Culture | The integrated pattern of human behaviour that includes thoughts, communications, actions, customs, beliefs, values, and institutions of a racial, ethnic, religious, or social group. | [29] |
| The accumulated socially acquired result of shared geography, time, ideas and human experience. Culture may or may not involve kinship, but meanings and understandings are collectively held by group members. Culture is dynamic and mobile and changes according to time, individuals and groups. | [30] | |
| There is a tendency within healthcare to equate culture with essentialized notions of race and ethnicity, which can lead to practices that separate culture from its social, economic and political context. Narrow conceptualizations of culture and identity may limit the effectiveness of particular approaches, and a focus on specific cultural information may inadvertently promote stereotyping. | [31] | |
| Cultural Awareness | a beginning step towards understanding that there is difference. Many people undergo courses designed to sensitise them to formal ritual rather than the emotional, social, economic and political context in which people exist | [30] |
| [is] concerned with having knowledge about cultural but, more specifically, ethnic diversity. | [32] | |
| an individual’s awareness of her/his own views such as ethnocentric, biased and prejudiced beliefs towards other cultures (p. e120) | [33] | |
| essentially the basic acknowledgment of differences between cultures | [34] | |
| recognizing that there are differences between cultures | [35] | |
| Cultural Sensitivity | alerts students to the legitimacy of difference and begins a process of self-exploration as the powerful bearers of their own life experience and realities and the impact this may have on others. | [30 |
| building on the awareness of difference through cultural acceptance, respect and understanding | [36] | |
| builds on cultural awareness’ acknowledgment of difference with the addition of the requirement of respecting other cultures | [34] | |
| where students start to analyse their own realities and the impact that this may have on others. | [35] | |
| Cultural Humility | incorporates a lifelong commitment to self-evaluation and self-critique, to redressing the power imbalances in the patient-physician dynamic, and to developing mutually beneficial and non-paternalistic clinical and advocacy partnerships with communities on behalf of individuals and defined populations. | [37] |
| entails valuing life-long learning and critical self-reflection, along with a respectful and inquisitive approach whereby practitioners are expected to seek knowledge from their clients regarding their cultural and structural influences rather than assuming understanding or expertise about a culture outside of their own | [38] | |
| defined as having an interpersonal stance that is other-oriented rather than self-focused, characterized by respect and lack of superiority toward an individual’s cultural background and experience. | [39] | |
| does not have an endpoint or goal; there is no objective of mastering another culture. Rather it is a continual process of self-reflection and self-critique that overtly addresses power inequities between providers and clients. Attaining cultural humility becomes not a goal but an active process, an ongoing way of being in the world and being in relationships with others and self. | [40] | |
| Cultural Security | it legitimises and values cultural differences to ensure no harm is caused and ultimately links understandings and actions | [41] |
| seeks to create interactions between health workers and health service users that do ‘not compromise the legitimate cultural rights, views, values and expectations of Aboriginal people’ | [42] | |
| Cultural Respect | The ‘Cultural Respect Framework for Aboriginal and Torres Strait Islander Health 2004–2009’ identifies the goal of cultural respect as ‘uphold[ing] the rights of Aboriginal and Torres Strait Islander peoples to maintain, protect and develop their culture and achieve equitable health outcomes | [42] |
| The model entails four basic elements highlighting the importance of ‘Knowledge and Awareness’ that informs ‘Skilled Practice and Behaviours’ as well as the development of ‘Strong Relationships’ between (health) institutions, individuals and communities in order to achieve an ‘Equity of Outcomes’ | [43] | |
| Cultural Adaptation | all modifications made to standard service methods in order to make services more acceptable, relevant, useful, and/or effective for diverse populations | [44] |
| Transcultural Competence | the ability to interact with clientele who come from a range of different cultural backgrounds | [43] |
| Transcultural Effectiveness | ability of organisations and systems ‘to acknowledge and respond to unique and diverse perspectives and support non- discriminatory practice’ (p. S51). These authors maintain, furthermore, that transculturally competent practitioners should recognise organisational and systemic obstacles and actively seek ways to modify them | [43] |
| Transcultural Nursing | Leininger (1994) defined transcultural nursing as being a subfield of nursing, focusing on comparative study and analysis of different cultures and is the basis on which the theory of culture care diversity and universality was formed. The goal of transcultural nurses being to “identify, test, understand and use a body of transcultural nursing knowledge and practices which is culturally derived in order to provide culturally specific nursing care to people” | [45] |
| Culturally Unsafe | “any actions that diminish, demean or disempower the cultural identity and well-being of an individual’ | [46, 47] |
| any action that diminishes, demeans, or disempowers the cultural identity and well-being of an individual | [48] | |
| Cultural Destructiveness | attitudes, policies, and practices that are destructive to cultures and consequently to the individuals within the culture such as cultural genocide | [29] |
| Cultural Incapacity | system or agencies that lack the capacity to help minority clients or communities due to extreme bias, paternalism and a belief in the racial superiority of the dominant group | [29] |
| Cultural Blindness | system or agencies that function with the belief that colour or culture make no difference and that all people are the same | [29] |
| Cultural Pre-competence | an agency that realises its weaknesses in serving minorities and attempts to improve some aspect of their services to a specific population | [29] |
| Cultural Proficiency | agencies that hold culture in high esteem, who seek to add to the knowledge base of culturally competent practice by conducting research and developing new therapeutic approaches based on culture | [29] |
One of the earliest [49] and most commonly cited definitions of cultural competency is sourced from a 1989 report authored by Cross and colleagues in the United States of America [29] (p.13):
Cultural competence is a set of congruent behaviours, attitudes, and policies that come together in a system, agency, or among professionals and enable that system, agency, or those professionals to work effectively in cross-cultural situations.
Cross et al. [29] contextualized cultural competency as part of a continuum ranging from the most negative end of cultural destructiveness (e.g. attitudes, policies, and practices that are destructive to cultures and consequently to the individuals within the culture such as cultural genocide) to the most positive end of cultural proficiency (e.g. agencies that hold culture in high esteem, who seek to add to the knowledge base of culturally competent practice by conducting research and developing new therapeutic approaches based on culture). Other points along this continuum include: cultural incapacity, cultural blindness and cultural pre-competence (Table 1).
By the time that cultural competency became to be better understood in the late 1990s, there had been substantial growth in the number of definitions, conceptual frameworks and related terms [31, 50,51,52]. Table 1 provides a summary of the multiple, interchangeable, terms such as: cultural awareness; cultural sensitivity; cultural humility; cultural security; cultural respect; cultural adaptation; and transcultural competence or effectiveness. Unfortunately, this rapid growth in terminology and theoretical positioning(s), further confused by variations in policy uptake across the health sector, reduced the potential for a common, shared understanding of what cultural competency represents and therefore what interventions are required. Table 2 outlines the various definitions of cultural competency from the literature.
Table 2 Key Definitions and Concepts of Cultural Competency
| Terms | Definition/ Concept Examples | Sources |
|---|---|---|
| Cultural Competency | a set of congruent behaviours, attitudes, and policies that come together in a system, agency, or among professionals and enable that system, agency, or those professionals to work effectively in cross-cultural situations. | [29] |
| acknowledges and incorporates - at all levels - the importance of culture, the assessment of cross-cultural relations, vigilance towards the dynamics that result from cultural differences, the expansion of cultural knowledge, and the adaptation of services to meet culturally-unique needs. | [29] | |
| a culturally competent counsellor must acquire ‘awareness, knowledge, and skills needed to function effectively in a pluralistic democratic society’, i.e., develop the ‘ability to communicate, interact, negotiate, and intervene on behalf of clients from diverse backgrounds | [43] | |
| the ability of individuals to establish effective interpersonal and working relationships that supersede cultural differences by recognizing the importance of social and cultural influences on patients, considering how these factors interact, and devising interventions that take these issues into account | [53] | |
| the ability of systems to provide care to patients with diverse values, beliefs and behaviours, including tailoring delivery to meet patients’ social, cultural, and linguistic needs | [54] | |
| a more comprehensive, skill-based concept that purposefully involves the system in addition to the patients and has been conceived of as an on-going quality improvement process, relevant across individual, organisational, systemic and professional levels | [50] | |
| a complex know-act grounded in critical reflection and action, which the health care professional draws upon to provide culturally safe, congruent, and effective care in partnership with individuals, families, and communities living health experiences, and which takes into account the social and political dimensions of care | [33] | |
| the ability to work and communicate effectively and appropriately with people from culturally different backgrounds. While appropriateness implies not violating the valued rules, effectiveness means achieving the valued goals and outcomes in intercultural interactions | [51] | |
| the ability to acknowledge, appreciate, and respect the values, preferences, and expressed needs of clients. Cultural competence is also the ability to resolve differences and identify solutions that reduce interference from various cultural factors…This article defines cultural competency as encompassing open-mindedness and a respect for people, families, and societies of various cultural backgrounds. Being able to translate this cultural knowledge and these skills into practice may help enhance the cultural appropriateness of healthcare. | [56] | |
| the development of a skill set for more effective provider-patient communication. They stressed the importance of providers’ understanding the relationship between cultural beliefs and behaviour and developing skills to improve quality of care to diverse populations. Several informants expressed concern about the persistence of stereotypic teaching strategies (such as treating Hispanics one way and African Americans another). They mentioned additional components that were underemphasized such as empathy, exploring socioeconomic issues, and addressing bias in the clinical encounter | [57] | |
| Social workers describe cultural competence as a continual process of striving to become increasingly self-aware, to value diversity, and to become knowledgeable about cultural strengths | [58] | |
| frequently approached in ways which limit its goals to knowledge of characteristics, cultural beliefs, and practices of different non-majority groups, and skills and attitudes of empathy and compassion in interviewing and communicating with non-majority groups. Achieving cultural competence is thus often viewed as a static outcome: One is “competent” in interacting with patients from diverse backgrounds much in the same way as one is competent in performing a physical exam or reading an EKG. | [23] | |
|
an awareness of cultural diversity and the ability to function effectively, and respectfully, when working with and treating people of different cultural backgrounds. Cultural competence means a doctor has the attitudes, skills and knowledge needed to achieve this. A culturally competent doctor will acknowledge:
|
[59] | |
| At the level of the individual practitioner, cultural competence enables increased awareness and understanding of the perspectives and lived realities of Māori clients, which in turn facilitates genuine engagement, trust, and information sharing contributing to enhanced clinical outcomes. | [54] | |
| Organisational Cultural Competency |
To achieve organizational cultural competence within the health care leadership and workforce, it is important to maximize diversity. This may be accomplished through:
|
[54] |
| Organisational cultural competence involves strategies that maximise diversity and incorporate leadership and workforce issues. Specifically, ethnic matching and working with communities. The lack of diversity in health care leadership and the workforce has been identified as a barrier to culturally competent care, and studies have shown that health care quality and racial and ethnic diversity are linked | ||
| Systemic Cultural Competency | To achieve systemic cultural competence (e.g., in the structures of the health care system) it is essential to address such initiatives as conducting community assessments, developing mechanisms for community and patient feedback, implementing systems for patient racial/ethnic and language preference data collection, developing quality measures for diverse patient populations, and ensuring culturally and linguistically appropriate health education materials and health promotion and disease prevention interventions. | [60] |
| At the system level, the structures of the health care system are attended to and include strategies, such as ethnicity data collection and strategic planning. Ethnicity data collection can assist in the planning of improvements to services by comparing access to services and outcomes of care. |
Cultural competence was often defined within an individually-focused framework, for example, as:
the ability of individuals to establish effective interpersonal and working relationships that supersede cultural differences by recognizing the importance of social and cultural influences on patients, considering how these factors interact, and devising interventions that take these issues into account [53] (p.2).
Some positionings for cultural competency have been critiqued for promoting the notion that health-care professionals should strive to (or even can) master a certain level of functioning, knowledge and understanding of Indigenous culture [61]. Cultural competency is limited when it focuses on acquiring knowledge, skills and attitudes as this infers that it is a ‘static’ level of achievement [58]:
“cultural competency” is frequently approached in ways which limit its goals to knowledge of characteristics, cultural beliefs, and practices of different nonmajority groups, and skills and attitudes of empathy and compassion in interviewing and communicating with nonmajority groups. Achieving cultural competence is thus often viewed as a static outcome: One is “competent” in interacting with patients from diverse backgrounds much in the same way as one is competent in performing a physical exam or reading an EKG. Cultural competency is not an abdominal exam. It is not a static requirement to be checked off some list but is something beyond the somewhat rigid categories of knowledge, skills, and attitudes (p.783).
By the early 2000s, governmental policies and cultural competency experts [50, 54] had begun to articulate cultural competency in terms of both individual and organizational interventions, and describe it with a broader, systems-level focus, e.g.:
the ability of systems to provide care to patients with diverse values, beliefs and behaviours, including tailoring delivery to meet patients’ social, cultural, and linguistic needs [54] (p. v)
Moreover, some commentators began to articulate the importance of critical reflection to cultural competency. For example, Garneau and Pepin [55] align themselves more closely to the notion of cultural safety when they describe cultural competency as:
a complex know-act grounded in critical reflection and action, which the health care professional draws upon to provide culturally safe, congruent, and effective care in partnership with individuals, families, and communities living health experiences, and which takes into account the social and political dimensions of care [55] (p. 12).
Reviewing Cultural Safety
A key difference between the concepts of cultural competency and cultural safety is the notion of ‘power’. There is a large body of work, developed over many years, describing the nuances of the two terms [34, 36, 38, 43, 46, 49, 59, 62, 63, 64, 65, 66, 67, 68, 69]. Similar to cultural competency, this concept has varying interpretations within and between countries. Table 3 summarises the definitions and use of cultural safety from the literature. Cultural safety foregrounds power differentials within society, the requirement for health professionals to reflect on interpersonal power differences (their own and that of the patient), and how the transfer of power within multiple contexts can facilitate appropriate care for Indigenous people and arguably for all patients [32].
Table 3: Key Definitions and Concepts of Cultural Safety
| Term | Definition/ Concept Examples | Sources |
|---|---|---|
| Cultural Safety | is an outcome of nursing and midwifery education that enables safe service to be defined by those that receive the service | [30] |
| a focus for the delivery of quality care through changes in thinking about power relationships and patients’ rights | [32] | |
| The skill for nurses and midwives does not lie in knowing the customs of ethnospecific cultures. Rather, cultural safety places an obligation on the nurse or midwife to provide care within the framework of recognizing and respecting the difference of any individual. But it is not the nurse or midwife who determines the issue of safety. It is consumers or patients who decide whether they feel safe with the care that has been given | [32] | |
| The focus of cultural safety teaching is to educate student nurses and student midwives: - to examine their own realities and the attitudes they bring to each new person they encounter in their practice; − to be open minded and flexible in their attitudes toward people who are different from themselves, to whom they offer or delivers - not to blame the victims of historical and social processes for their current plight; − to produce a workforce of well educated, self-aware registered nurses and midwives who are culturally safe to practice |
[32] | |
| where there is no inadvertent disempowering of the recipient, indeed where recipients are involved in the decision making and become part of a team effort to maximise the effectiveness of the care. The model pursues more effective practice through being aware of difference, decolonising, considering power relationships, implementing reflective practice, and by allowing the patient to determine what safety means. | [65] | |
| a nurse who could objectively evaluate his or her own culture and be familiar about the theory of power structures, is also a culturally safe nurse in all contexts | [35] | |
| places an emphasis on the health worker understanding their own culture and identity, and how this manifests in their practice. Thus, cultural safety is concerned with both systemic and individual change with the aim of examining processes of identity formation and enhancing health workers’ awareness of their own identity and its impact on the care they provide to people from indigenous cultural groups. | [42] | |
| aims to directly address the effects of colonialism within the dominant health system by focusing on the level of cultural safety felt by an individual seeking health care. The responsibility to recognize and protect a person’s cultural identity (and hence maintain their cultural safety) lies with the health service. Emphasis is placed on assisting the health worker to understand processes of identity and culture, and how power imbalances or relationships can be culturally unsafe (and thus, detrimental to a person’s health and wellbeing) | [42] | |
| a strategic and intensely practical plan to change the way healthcare is delivered to Aboriginal people. In particular, the concept is used to express an approach to healthcare that recognizes the contemporary conditions of Aboriginal people which result from their post-contact history. | [63] | |
| the movement from cultural competence to cultural safety is not merely another step on a linear continuum, but rather a more dramatic change of approach. This conceptualization of cultural safety represents a more radical, politicized understanding of cultural consideration, effectively rejecting the more limited culturally competent approach for one based not on knowledge but rather on power. | [63] | |
| best nurtured in conjunction with other embedded philosophies such as decolonization, symbolic interactionism, understanding social interaction in context, and the social justice imperative to avoid further harm from domination and oppression | [47] | |
| a constant self-evaluation by a provider to ensure they’re focusing on the individual and are not being influenced by assumptions about that individual’s cultural background or social or economic status…also helps alter the colonial relationship and makes safe space for Indigenous peoples within the system and thereby allowing them to help reshape the system itself | [62] | |
| provides for the formal recognition of power relations within health care (and in particular nursing) interactions. By adopting cultural safety it becomes not only possible but inevitable that an exploration of the assumptions underlying practice, brought by both individuals and the profession will occur. This reflective model is effective on the individual, institutional and professional levels, and encourages identification of the assumptions and preconceptions that structure practice | [66] | |
| a powerful means of conveying the idea that cultural factors critically influence the relationship between carer and patient. Cultural safety focuses on the potential differences between health providers and patients that have an impact on care and aims to minimize any assault on the patient’s cultural identity. Specifically, the objectives of cultural safety in nursing and midwifery training are to educate students to examine their own realities and attitudes they bring to clinical care, to educate them to be open-minded towards people who are different from themselves, to educate them not to blame the victims of historical and social processes for their current plight, and to produce a workforce of well-educated and self-aware health professionals who are culturally safe to practice as defined by the people they serve. | [46] | |
| does not emphasize developing “competence” through knowledge about the cultures with which professionals are working. Instead, cultural safety emphasizes recognizing the social, historical, political and economic circumstances that create power differences and inequalities in health and the clinical encounter | [46] | |
| is underpinned by a social justice framework and requires individuals to undertake a process of personal reflection. Cultural safety is therefore a holistic and shared approach, where all individuals feel safe, can undertake learning [36] together with dignity, and demonstrate deep listening | [36] | |
| is grounded in critical theoretical perspectives and draws attention to critically oriented knowledge, such as racialization, culturalism, institutional racism and discrimination, and health and health care inequities | [68] | |
| extends beyond cultural awareness, sensitivity, and skills-based competencies and is predicated on understanding the power differentials inherent in health care service delivery to redress these inequities through educational processes, focusing on reflexive thinking | [70] | |
| is informed philosophically by “emancipatory or neocolonisation theoretical perspectives” and by an emphasis on social justice. Grounded in critical theory, cultural safety invites the nurse | [71] | |
| goes beyond describing the practices of other ethnic groups, because such a strategy can lead to a checklist mentality that essentialises group members. Furthermore, a nurse having knowledge of a client’s culture could be disempowering for a client who is disenfranchised from their own culture, and could be seen as the continuation of a colonising process that is both demeaning and disempowering or appropriating. Culturally safe nurses focus on self-understanding and the emphasis is on what attitudes and values nurses bring to their practice. A key tenet is that ‘a nurse or midwife who can understand his or her own culture and the theory of power relations can be culturally safe in any context’ | [60] | |
| advocates that both professionals and institutions work to establish a safe place for patients, which is sensitive and responsive to their social, political, linguistic, economic and spiritual concerns. Cultural safety is more than an understanding of a patient’s ethnic background as it requires the ‘health professional to reflect on their own cultural identity and on their relative power as a health provider’ | [72] | |
| The curriculum staircase or poutama assumes that students begin their cultural safety education at the bottom of the staircase where they bring with them their personal experiences, knowledge, and biases. Over the next 3 years of their training, the students are assessed on their ability to move to each step. This training focuses on racism awareness, the Treaty of Waitangi, ngā mea Māori (concepts important to Māori), and strategies for institutional change. Hence, the educational process involves movement from awareness to sensitivity, and ultimately to safety. | [48] | |
| we envisioned that cultural safety might assist nurses to examine how popularized notions of culture and cultural differences are taken up; to develop greater awareness of how individual and societal assumptions and stereotypes operate in practice; and to better recognize how organizational and structural inequities and wider social discourses – within health care and in our society – inevitably influence nurses’ interpretive perspectives and practices. | [73] | |
| Critical Consciousness | If we try to move beyond cultural competency and instead focus on the development of this critical consciousness, what is its object of knowledge? In other words, “What stuff should we learn?” The object of knowledge is not just a series of lists of cultural attributes (which can quickly degrade into dehumanizing stereotypes), nor is it a skill set of questions and demeanours we should assume when encountering a patient who is not like us. We propose that the object of knowledge of these educational efforts is the development of critical consciousness itself, that is, the knowledge and awareness to carry out the social roles and responsibilities of a physician. This way of knowing is a different type of knowledge than that required when studying the biomedical sciences— complementary, but different all the same. | [58] |
| Cultural competency is not an abdominal exam. It is not a static requirement to be checked off some list but is something beyond the somewhat rigid categories of knowledge, skills, and attitudes: the continuous critical refinement and fostering of a type of thinking and knowing—a critical consciousness— of self, others, and the world. | [58] |
The term cultural safety first was first proposed by Dr. Irihapeti Ramsden and Māori nurses in the 1990s [74], and in 1992 the Nursing Council of New Zealand made cultural safety a requirement for nursing and midwifery education [32]. Cultural safety was described as providing:
a focus for the delivery of quality care through changes in thinking about power relationships and patients’ rights [32]. (p.493).
Cultural safety is about acknowledging the barriers to clinical effectiveness arising from the inherent power imbalance between provider and patient [65]. This concept rejects the notion that health providers should focus on learning cultural customs of different ethnic groups. Instead, cultural safety seeks to achieve better care through being aware of difference, decolonising, considering power relationships, implementing reflective practice, and by allowing the patient to determine whether a clinical encounter is safe [32, 65].
Cultural safety requires health practitioners to examine themselves and the potential impact of their own culture on clinical interactions. This requires health providers to question their own biases, attitudes, assumptions, stereotypes and prejudices that may be contributing to a lower quality of healthcare for some patients. In contrast to cultural competency, the focus of cultural safety moves to the culture of the clinician or the clinical environment rather than the culture of the ‘exotic other’ patient.
There is debate over whether cultural safety reflects an end point along a continuum of cultural competency development, or, whether cultural safety requires a paradigm shift associated with a transformational jump in cultural awareness. Dr. Irihapeti Ramsden [75] originally described the process towards achieving cultural safety in nursing and midwifery practice as a step-wise progression from cultural awareness through to cultural sensitivity and on to cultural safety. However, Ramsden was clear that the terms cultural awareness and cultural sensitivity were separate concepts and that they were not interchangeable with cultural safety. Despite some authors interpreting Ramsden’s original description of cultural safety as involving three steps along a continuum [35] other authors view a move to cultural safety as more of a ‘paradigm shift’ [63]:
where the movement from cultural competence to cultural safety is not merely another step on a linear continuum, but rather a more dramatic change of approach. This conceptualization of cultural safety represents a more radical, politicized understanding of cultural consideration, effectively rejecting the more limited culturally competent approach for one based not on knowledge but rather on power [63]. (p.10).
Regardless of whether cultural safety represents movement along a continuum or a paradigm shift, commentators are clear that the concept of cultural safety aligns with critical theory, where health providers are invited to “examine sources of repression, social domination, and structural variables such as class and power” [71] (p.144) and “social justice, equity and respect” [76] (p.1). This requires a movement to critical consciousness, involving critical self-reflection: “a stepping back to understand one’s own assumptions, biases, and values, and a shifting of one’s gaze from self to others and conditions of injustice in the world.” [58] (p.783).
Why a Narrow Understanding of Cultural Competency may be Harmful
Unfortunately, regulatory and educational health organisations have tended to frame their understanding of cultural competency towards individualised rather than organisational/systemic processes, and on the acquisition of cultural-knowledge rather than reflective self-assessment of power, priviledge and biases. There are a number of reasons why this approach can be harmful and undermine progress on reducing health inequities.
Individual-level focused positionings for cultural competency perpetuate a process of “othering”, that identifies those that are thought to be different from oneself or the dominant culture. The consequences for persons who experience othering include alienation, marginalization, decreased opportunities, internalized oppression, and exclusion [77]. To foster safe and effective health care interactions, those in power must actively seek to unmask othering practices [78].
“Other-focused” approaches to cultural competency promote oversimplified understandings of other cultures based on cultural stereotypes, including a tendency to homogenise Indigenous people into a collective ‘they’ [79]. This type of cultural essentialism not only leads to health care providers making erroneous assumptions about individual patients which may undermine the provision of good quality care [31, 53, 58, 63, 64], but also reinforces a racialised, binary discourse, used to repeatedly dislocate and destabilise Indigenous identity formations [80]. By ignoring power, narrow approaches to cultural competency perpetuate deficit discourses that place responsibility for problems with the affected individuals or communities [81], overlooking the role of the health professional, the health care system and broader socio-economic structures. Inequities in access to the social determinants of health have their foundations in colonial histories and subsequent imbalances in power that have consistently benefited some over others. Health equity simply cannot be achieved without acknowledging and addressing differential power, in the healthcare interaction, and in the broader health system and social structures (including in decision making and resource allocation) [82].
An approach to cultural competency that focuses on acquiring knowledge, skills and attitudes is problematic because it suggests that competency can be fully achieved through this static process [58]. Cultural competency does not have an endpoint, and a “tick-box” approach may well lull practitioners into a falsely confident space. These dangers underscore the importance of framing cultural safety as an ongoing and reflective process, focused on ‘critical consciousness’. There will still be a need for health professionals to have a degree of knowledge and understanding of other cultures, but this should not be confused with or presented as efforts to address cultural safety. Indeed, as discussed above, this information alone can be dangerous without deep self-reflection about how power and privilege have been redistributed during those processes and the implications for our systems and practice.
By neglecting the organisational/systemic drivers of health care inequities, individual-level focused positionings for cultural competency are fundementally limited in their ability to impact on health inequities. Healthcare organisations influence health provider bias through the structure of the healthcare environment, including factors such as their commitment to workforce training, accountability for equity, workplace stressors, and diversity in workforce and governance [27]. Working towards cultural safety should not be viewed as an intervention purely at the level of the health professional – although a critically conscious and empathetic health professional is certainly important. The evidence clearly emphasises the important role that healthcare organisations (and society at large) can have in the creation of culturally safe environments [31, 32, 46, 60, 69]. Cultural safety initiatives therefore should target both individual health professionals and health professional organisations to intervene positively towards achieving health equity.
Perhaps not surprisingly, the concept of cultural safety is often more confronting and challenging for health institutions, professionals, and students than that of cultural competency. Regardless, it has become increasingly clear that health practitioners, healthcare organisations and health systems all need to be engaged in working towards cultural safety and critical consciousness. To do this, they must be prepared to critique the ‘taken for granted’ power structures and be prepared to challenge their own culture, biases, privilege and power rather than attempt to become ‘competent’ in the cultures of others.
Redefining Cultural Safety to Achieve Health Equity
It is clear from reviewing the current evidence associated with cultural competency and cultural safety that a shift in approach is required. We recommend an approach to cultural safety that encompasses the following core principles:
- Be clearly focused on achieving health equity, with measureable progress towards this endpoint;
- Be centred on clarified concepts of cultural safety and critical consciousness rather than narrow based notions of cultural competency;
- Be focused on the application of cultural safety within a healthcare systemic/organizational context in addition to the individual health provider-patient interface;
- Focus on cultural safety activities that extend beyond acquiring knowledge about ‘other cultures’ and developing appropriate skills and attitudes and move to interventions that acknowledge and address biases and stereotypes;
- Promote the framing of cultural safety as requiring a focus on power relationships and inequities within health care interactions that reflect historical and social dynamics.
- Not be limited to formal training curricula but be aligned across all training/practice environments, systems, structures, and policies.
We recommend that the following definition for cultural safety is adopted by healthcare organisations:
Cultural safety requires healthcare professionals and their associated healthcare organisations to examine themselves and the potential impact of their own culture on clinical interactions and healthcare service delivery. This requires individual healthcare professionals and healthcare organisations to acknowledge and address their own biases, attitudes, assumptions, stereotypes, prejudices, structures and characteristics that may affect the quality of care provided. In doing so, cultural safety encompasses a critical consciousness where healthcare professionals and healthcare organisations engage in ongoing self-reflection and self-awareness and hold themselves accountable for providing culturally safe care, as defined by the patient and their communities, and as measured through progress towards acheiveing health equity. Cultural safety requires healthcare professionals and their associated healthcare organisations to influence healthcare to reduce bias and achieve equity within the workforce and working environment.
In operationalising this approach to cultural safety, organisations (health professional training bodies, healthcare organisations etc) should begin with a self-review of the extent to which they meet expectations of cultural safety at a systemic and organizational level and identify an action plan for development. The following steps should also be considered by healthcare organisations and regulators to take a more comprehensive approach to cultural safety:
- Mandate evidence of engagement and transformation in cultural safety activities as a part of vocational training and professional development;
- Include evidence of cultural safety (of organisations and practitioners) as a requirement for accreditation and ongoing certification;
- Ensure that cultural safety is assessed by the systematic monitoring and assessment of inequities (in health workforce and health outcomes);
- Require cultural safety training and performance monitoring for staff, supervisors and assessors;
- Acknowledge that cultural safety is an independent requirement that relates to, but is not restricted to, expectations for competency in ethnic or Indigenous health.
Conclusion
Cultural competency, cultural safety and related terms have been variably defined and applied. Unfortunately, regulatory and educational health organisations have tended to frame their understanding of cultural competency towards individualised rather than organisational/systemic processes, and on the acquisition of cultural-knowledge rather than reflective self-assessment of power, priviledge and biases. This positioning has limited the impact on improving health inequities. A shift is required to an approach based on a transformative concept of cultural safety, which involves a critique of power imbalances and critical self-reflection.
Health practitioners, healthcare organisations and health systems need to be engaged in working towards cultural safety and critical consciousness. To do this, they must be prepared to critique the ‘taken for granted’ power structures and be prepared to challenge their own culture and cultural systems rather than prioritise becoming ‘competent’ in the cultures of others. The objective of cultural safety activities also needs to be clearly linked to achieving health equity. Healthcare organisations and authorities need to be held accountable for providing culturally safe care, as defined by patients and their communities, and as measured through progress towards achieving health equity.
We propose principles and a definition for cultural safety that addresses the key factors identified as being responsible for ethnic inequities in health care, and which we therefore believe is fit for purpose in Aotearoa New Zealand and internationally. We hope this will be a useful starting point for users to further reflect on the work required for themselves, and their organisations, to contribute to the creation of culturally safe environments and therefore to the elimination of Indigenous and ethnic health inequities. More work is needed on how best to train and monitor for cultural safety within health workforce contexts.
References
- Anderson I, et al. Indigenous and tribal peoples’ health (the lancet–Lowitja Institute global collaboration): a population study. Lancet. 2016;388(10040):131–57.
- Smedley B, Stith A, Nelson A. Eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. 2002. National Academy Press: Washington.
- Pigou, P. and N. Joseph, Programme Scope: Cultural competence, partnership and health equity. 2017, New Zealand Medical Council of New Zealand and Te Ohu Rata O Aotearoa: Wellington. p. 1–9.
- Statistics New Zealand. Life Expectancy. NZ Social Indicators 2015 [cited 2016 January 7]; Available from: http://www.stats.govt.nz/browse_for_stats/snapshots-of-nz/nz-social-indicators/Home/Health/life-expectancy.aspx.
- Jansen P, Jansen D. Māori and health, in Cole's medical practice in New Zealand, I.M. St George, editor. 2013. Medical Council of New Zealand: Wellington.
- Ministry of Health, Tatau Kahukura: Māori Health Chart Book. 2006, Ministry of Health: Wellington.
- Davis P, et al. Quality of hospital care for Maori patients in New Zealand: retrospective cross-sectional assessment. Lancet. 2006;367(9526):1920–5.
- Ministry of Health, Tatau Kahukura: Māori Health Chart Book 2015 (3rd edition). 2015, Ministry of Health: Wellington.
- Metcalfe S, et al. Te Wero tonu-the challenge continues: Māori access to medicines 2006/07-2012/13 update. - PubMed - NCBI. N Z Med J. 2018;131(1485):27–47.
- Health Quality & Safety Commission, A Window on the Quality of New Zealand’s Health Care 2017. 2017, Wellington, New Zealand: Health Quality & Safety Commission.
- Reid P, et al. Achieving health equity in Aotearoa: strengthening responsiveness to Māori in health research. The New Zealand Medical Journal. 2017;130(1465):96–103.
- United Nations. United Nations Declaration on the Rights of Indigenous peoples, U. Nations, editor. 2008. United Nations: Geneva.
- Robson B, Harris R. Eds. Hauora: Māori Standards of Health IV. A study of the years 2000-2005. 2007. Te Rōpū Rangahau Hauora a Eru Pōmare: Wellington.
- World Health Organisation, Commission on Social Determinants of Health. Final report. 2008, World Health Organization: Geneva.
- Reid, P. and B. Robson, Understanding Health Inequities, in Hauora: Māori Standards of Health IV. A study of the years 2000–2005, B. Robson and R. Harris, Editors. 2007, Te Rōpū Rangahau Hauora a Eru Pōmare: Wellington. p. 3–10.
- Krieger, N., Theories for social epidemiology in the 21st century: an ecodocial perspective. Int J Epidemiol, 2001: p. 668–677.
- Reid P, Robson B, Jones CP. Disparities in health: common myths and uncommon truths. Pacific Health Dialog. 2000;7(1):38–47.
- Cooper L, et al. Delving below the surface. Understanding how race and ethnicity influence relationships in health care. J Gen Intern Med. 2006;21(Suppl. 1):21–7.
- van Ryn M, Fu S. Paved with good intentions: do public health and human service providers contribute to racial/ethnic disparities in health? Am J Public Health. 2003;93(2):248–55.
- van Ryn M, Saha S. Exploring unconscious Bias in disparities research and medical education. J Am Med Assoc. 2011;306(9):995–6.
- Health Practitioners Competence Assurance Act 2003, in 2003 No 48. 2003: New Zealand.
- Canadian Nurses Association, Position statement: promoting culturally competent care. 2004, Canadian nurses association,. Ottawa.
- Medical Council of New Zealand, Statement on cultural competence. 2006, Medical Council of New Zealand: Wellington.
- Medical Board of Australia, Good medical practice: a code of conduct for doctors in Australia. . 2014, Medical Board of Australia.
- Nursing Council of New Zealand, Guidelines for Cultural Safety, the Treaty of Waitangi and Maori Health in Nursing Education and Practice. 2011, Nursing Council of New Zealand,.
- Reid, P. and R. Jones, Cultural Competence and Māori Health. MCNZ/Te ORA Cultural Competence Symposium held on 17th November 2017 (powerpoint). 2017: Wellington.
- van Ryn M, et al. The impact of racism on clinician cognition, behavior, and clinical decision making. Du Bois Review: Social Science Research on Race. 2011;8(1):199–218.
- Curtis E. Indigenous positioning in health research: the importance of Kaupapa Māori theory informed practice. AlterNative: An International Journal of Indigenous Peoples. 2016;12(4):396.
- Cross, T., B. Bazron, and M. lsaccs, Towards a Culturally Competent System of Care: A Monograph on Effective Services for Minority Children Who Are Severely Emotionally Disturbed. CASSP technical assistance Centre. Washington DC: Georgetown University Child Development Center; 1989.
- Ramsden, I., Cultural Safety and Nursing Education in Aotearoa and Te Waipounamu. A thesis submitted to the Victoria University of Wellington in fulfilment of the requirements for the degree of Doctor of Philosophy in Nursing, in Department of Nursing. 2002, Victoria University of Wellington Wellington. p. 211.
- Truong M, Paradies Y, Priest N. Interventions to improve cultural competency in healthcare: a systematic review of reviews. BMC Health Serv Res. 2014;14:99.
- Papps E, Ramsden I. Cultural safety in nursing: the New Zealand experience. Int J Qual Health Care. 1996;8(5):491–7.
- Alizadeh S, Chavan M. Cultural competence dimensions and outcomes: a systematic review of the literature. Health & Social Care in the Community. 2016;24(6):e117–30.
- Darroch F, et al. The United States does CAIR about cultural safety: examining cultural safety within indigenous health contexts in Canada and United States. J Transcult Nurs. 2017;28(3):269–77.
- Eriksson, C. and L. Eriksson, Inequities in health care: lessons from New Zealand : A qualitative interview study about the cultural safety theory. 2017. p. 31.
- Milne, T., D.K. Creedy, and R. West, Development of the Awareness of Cultural Safety Scale: A pilot study with midwifery and nursing academics. Nurse Education Today, 2016. 44(Supplement C): p. 20–25.
- Tervalon M, Murray-García J. Cultural humility versus cultural competence: a critical distinction in defining physician training outcomes in multicultural education. J Health Care Poor Underserved. 1998;9(2):117–25.
- McLennan V, et al. Creating culturally safe vocational rehabilitation services for indigenous Australians: a brief review of the literature. Australian Journal of Rehabilitation Counselling. 2016;22(2):93–103.
- Hook JN, et al. Cultural humility: measuring openness to culturally diverse clients. J Couns Psychol. 2013;60(3):353–66.
- Miller S. Cultural humility is the first step to becoming global care providers. JOGNN - Journal of Obstetric, Gynecologic, and Neonatal Nursing. 2009;38(1):92–3.
- Phiri J, Dietsch E, Bonner A. Cultural safety and its importance for Australian midwifery practice. Collegian. 2010;17(3):105–11.
- Downing R, Kowal E, Paradies Y. Indigenous cultural training for health workers in Australia. Int J Qual Health Care. 2011;23(3):247–57.
- Grote E. Principles and practices of cultural competency: a review of the literature. Indigenous Higher Education Advisory Council (IHEAC), Australian Government, Department of Education Employment and Workplace Relations: Canberra; 2008.
- Healey P, et al. Cultural adaptations to augment health and mental health services: a systematic review. BMC Health Serv Res. 2017;17(1):1–26.
- Gibbs KA. Teaching student nurses to be culturally safe: can it be done? J Transcult Nurs. 2005;16(4):356–60.
- Kirmayer LJ. Rethinking cultural competence. Transcultural Psychiatry. 2012;49(2):149–64.
- Blanchet-Cohen, N. And C. Richardson/Kinewesquao, Foreword: fostering cultural safety across contexts. AlterNative: An International Journal of Indigenous Peoples, 2017. 13(3): p. 138–141.
- Wepa D. An exploration of the experiences of cultural safety educators in New Zealand: an action research approach. J Transcult Nurs. 2003;14(4):339–48.
- Shen Z. Cultural competence models and cultural competence assessment instruments in nursing: a literature review. J Transcult Nurs. 2015;26(3):308–21.
- Horvat L, et al. Cultural competence education for health professionals. Cochrane Database Syst Rev. 2014;5:CD009405.
- Lin CJ, Lee CK, Huang MC. Cultural competence of healthcare providers: a systematic review of assessment instruments. J Nurs Res. 2017;25(3):174–86.
- Leininger M. Culture care theory: a major contribution to advance transcultural nursing knowledge and practices. J Transcult Nurs. 2002;13(3):189–92.
- Beach MC, et al. Cultural competence: a systematic review of health care provider educational interventions. Med Care. 2005;43(4):356–73.
- Betancourt J, Green A, Carillo J. Cultural Competence in Health Care: Emerging Frameworks and Practical Approaches. 2002. The Commonwealth Fund: New York.
- Garneau AB, Pepin J. Cultural competence: a constructivist definition. J Transcult Nurs. 2015;26(1):9–15.
- Betancourt J, et al. Cultural competence and health care disparities: key perspectives and trends. Health Aff. 2005;24(2):499–505.
- Maier-Lorentz MM. Transcultural nursing: its importance in nursing practice. J Cult Divers. 2008;15(1):37–43.
- Kumagai A, Lypson M. Beyond cultural competence: critical consciousness, social justice, and multicultural education. Acad Med. 2009;84(6):782–7.
- Ratima M, Waetford C, Wikaire E. Cultural competence for physiotherapists: reducing inequalities in health between Maori and non-Maori. N Z J Physiother. 2006;34(3):153–9.
- DeSouza R. Wellness for all: the possibilities of cultural safety and cultural competence in New Zealand. J Res Nurs. 2008;13(2):125–35.
- Duke, J.A.N., M. Connor, And R. McEldowney, Becoming a culturally competent health practitioner in the delivery of culturally safe care: a process oriented approach Journal of Cultural Diversity, 2009. 16(2): p. 40–49.
- Ringer J. Cultural safety and engagement: keys to improving access to care. Healthcare Management Forum. 2017;30(4):213–7.
- Brascoupé, S. And C.B.a.M.a. waters, Cultural Safety: Exploring the Applicability of the Concept of Cultural Safety to Aboriginal Health and Community Wellness. J Aborig Health, 2009. 5(2): p. 6–41.
- Polaschek NR. Cultural safety: a new concept in nursing people of different ethnicities. J Adv Nurs. 1998;27:452–7.
- Laverty M, McDermott DR, Calma T. Embedding cultural safety in Australia’s main health care standards. Med J Aust. 2017;207(1):15–6.
- Richardson, A., J. Yarwood, and S. Richardson, Expressions of cultural safety in public health nursing practice. Nurs Inq, 2017. 24(1).
- Wilson D, Neville S. Culturally safe research with vulnerable populations. Contemp Nurse. 2009;33(1):69–79.
- Blanchet Garneau, A., et al., Applying cultural safety beyond Indigenous contexts: Insights from health research with Amish and Low German Mennonites. Nurs Inq, 2018. 25(1).
- Main C, McCallin A, Smith N. Cultural safety and cultural competence: what does this mean for physiotherapists? N Z J Physiother. 2006;34(3):160–6.
- Rowan, M.S., et al., Cultural competence and cultural safety in Canadian Schools of Nursing: A mixed methods study. Int J Nurs Educ Scholarsh, 2013. 10(1).
- Doutrich D, et al. Cultural safety in New Zealand and the United States: looking at a way forward together. J Transcult Nurs. 2012;23(2):143–50.
- McGough S, Wynaden D, Wright M. Experience of providing cultural safety in mental health to aboriginal patients: a grounded theory study. Int J Ment Health Nurs. 2018;27(1):204–13.
- Browne A, Varcoe C, Smye V, Reimer-Kirkham S, Lynam J, Wong S. Cultural safety and the challenges of translating critically oriented knowledge in practice. Nurs Philos. 2009;10:167.
- Ramsden, I., Towards cultural safety, in Cultural Safety in Aotearoa New Zealand. Second edition, D. Wepa, Editor. 2015, Cambridge University Press: Melbourne. p. 5–25.
- Ramsden I. Cultural Safety and Nursing Education in Aotearoa and Te Waipounamu, in Nursing. Victoria University of Wellington: Wellington; 2002.
- McGough, S., D. Wynaden, and M. Wright, Experience of providing cultural safety in mental health to aboriginal patients: a grounded theory study. International Journal of Mental Health Nursing, 2017.
- Canales MK. Othering: toward an understanding of difference. Adv Nurs Sci. 2019;22(4):16–31.
- Johnson JL, et al. Othering and being othered in the context of health care services. - PubMed - NCBI. Health Commun. 2019;16(2):255–71.
- MacNaughton G, Davis K. Beyond 'Othering': rethinking approaches to teaching young Anglo-Australian children about indigenous Australians; 2001.
- McGrath S. Binary discourses and 'othering' indigenous Australians; 2017.
- Fogarty W, et al. Deficit discourse and indigenous health: how narrative framings of aboriginal and Torres Strait islander people are reproduced in policy. Melbourne: The Lowitja Institute; 2018.
- Givens, M., et al., Power: the Most fundamental cause of health inequity? . Health Affairs Blog, 2018.

McIntosh, P. (2011). White privilege: Unpacking the invisible knapsack. In M. B. Bukelew & A. Fishman (Eds.) Reaching and teaching diverse populations: Strategies for moving beyond stereotypes (pp. 71-74). SAGE Publications.
Through work to bring materials from women's studies into the rest of the curriculum, I have often noticed men's unwillingness to grant that they are over-privileged, even though they may grant that women are disadvantaged. They may say they will work to women's statues, in the society, the university, or the curriculum, but they can't or won't support the idea of lessening men's. Denials that amount to taboos surround the subject of advantages that men gain from women's disadvantages. These denials protect male privilege from being fully acknowledged, lessened, or ended.
Thinking through unacknowledged male privilege as a phenomenon, I realized that, since hierarchies in our society are interlocking, there was most likely a phenomenon of while privilege that was similarly denied and protected. As a white person, I realized I had been taught about racism as something that puts others at a disadvantage, but had been taught not to see one of its corollary aspects, white privilege, which puts me at an advantage.
I think whites are carefully taught not to recognize white privilege, as males are taught not to recognize male privilege. So I have begun in an untutored way to ask what it is like to have white privilege. I have come to see white privilege as an invisible package of unearned assets that I can count on cashing in each day, but about which I was "meant" to remain oblivious. White privilege is like an invisible weightless knapsack of special provisions, maps, passports, codebooks, visas, clothes, tools, and blank checks.
Describing white privilege makes one newly accountable. As we in women's studies work to reveal male privilege and ask men to give up some of their power, so one who writes about having white privilege must ask, "having described it, what will I do to lessen or end it?" After I realized the extent to which men work from a base of unacknowledged privilege, I understood that much of their oppressiveness was unconscious. Then I remembered the frequent charges from women of color that white women whom they encounter are oppressive. I began to understand why we are just seen as oppressive, even when we don't see ourselves that way. I began to count the ways in which I enjoy unearned skin privilege and have been conditioned into oblivion about its existence.
My schooling gave me no training in seeing myself as an oppressor, as an unfairly advantaged person, or as a participant in a damaged culture. I was taught to see myself as an individual whose moral state depended on her individual moral will. My schooling followed the pattern my colleague Elizabeth Minnich has pointed out: whites are taught to think of their lives as morally neutral, normative, and average, and also ideal, so that when we work to benefit others, this is seen as work that will allow "them" to be more like "us."
Daily Effects of White Privilege
I decided to try to work on myself at least by identifying some of the daily effects of white privilege in my life. I have chosen those conditions that I think in my case attach somewhat more to skin-color privilege than to class, religion, ethnic status, or geographic location, though of course all these other factors are intricately intertwined. As far as I can tell, my African American co-workers, friends, and acquaintances with whom I come into daily or frequent contact in this particular time, place and time of work cannot count on most of these conditions.
- I can if I wish arrange to be in the company of people of my race most of the time.
- I can avoid spending time with people whom I was trained to mistrust and who have learned to mistrust my kind or me.
- If I should need to move, I can be pretty sure of renting or purchasing housing in an area which I can afford and in which I would want to live.
- I can be pretty sure that my neighbors in such a location will be neutral or pleasant to me.
- I can go shopping alone most of the time, pretty well assured that I will not be followed or harassed.
- I can turn on the television or open to the front page of the paper and see people of my race widely represented.
- When I am told about our national heritage or about "civilization," I am shown that people of my color made it what it is.
- I can be sure that my children will be given curricular materials that testify to the existence of their race.
- If I want to, I can be pretty sure of finding a publisher for this piece on white privilege.
- I can be pretty sure of having my voice heard in a group in which I am the only member of my race.
- I can be casual about whether or not to listen to another person's voice in a group in which s/he is the only member of his/her race.
- I can go into a music shop and count on finding the music of my race represented, into a supermarket and find the staple foods which fit with my cultural traditions, into a hairdresser's shop and find someone who can cut my hair.
- Whether I use checks, credit cards or cash, I can count on my skin color not to work against the appearance of financial reliability.
- I can arrange to protect my children most of the time from people who might not like them.
- I do not have to educate my children to be aware of systemic racism for their own daily physical protection.
- I can be pretty sure that my children's teachers and employers will tolerate them if they fit school and workplace norms; my chief worries about them do not concern others' attitudes toward their race.
- I can talk with my mouth full and not have people put this down to my color.
- I can swear, or dress in second hand clothes, or not answer letters, without having people attribute these choices to the bad morals, the poverty or the illiteracy of my race.
- I can speak in public to a powerful male group without putting my race on trial.
- I can do well in a challenging situation without being called a credit to my race.
- I am never asked to speak for all the people of my racial group.
- I can remain oblivious of the language and customs of persons of color who constitute the world's majority without feeling in my culture any penalty for such oblivion.
- I can criticize our government and talk about how much I fear its policies and behavior without being seen as a cultural outsider.
- I can be pretty sure that if I ask to talk to the "person in charge", I will be facing a person of my race.
- If a traffic cop pulls me over or if the IRS audits my tax return, I can be sure I haven't been singled out because of my race.
- I can easily buy posters, post-cards, picture books, greeting cards, dolls, toys and children's magazines featuring people of my race.
- I can go home from most meetings of organizations I belong to feeling somewhat tied in, rather than isolated, out-of-place, outnumbered, unheard, held at a distance or feared.
- I can be pretty sure that an argument with a colleague of another race is more likely to jeopardize her/his chances for advancement than to jeopardize mine.
- I can be pretty sure that if I argue for the promotion of a person of another race, or a program centering on race, this is not likely to cost me heavily within my present setting, even if my colleagues disagree with me.
- If I declare there is a racial issue at hand, or there isn't a racial issue at hand, my race will lend me more credibility for either position than a person of color will have.
- I can choose to ignore developments in minority writing and minority activist programs, or disparage them, or learn from them, but in any case, I can find ways to be more or less protected from negative consequences of any of these choices.
- My culture gives me little fear about ignoring the perspectives and powers of people of other races.
- I am not made acutely aware that my shape, bearing or body odor will be taken as a reflection on my race.
- I can worry about racism without being seen as self-interested or self-seeking.
- I can take a job with an affirmative action employer without having my co-workers on the job suspect that I got it because of my race.
- If my day, week or year is going badly, I need not ask of each negative episode or situation whether it had racial overtones.
- I can be pretty sure of finding people who would be willing to talk with me and advise me about my next steps, professionally.
- I can think over many options, social, political, imaginative or professional, without asking whether a person of my race would be accepted or allowed to do what I want to do.
- I can be late to a meeting without having the lateness reflect on my race.
- I can choose public accommodation without fearing that people of my race cannot get in or will be mistreated in the places I have chosen.
- I can be sure that if I need legal or medical help, my race will not work against me.
- I can arrange my activities so that I will never have to experience feelings of rejection owing to my race.
- If I have low credibility as a leader I can be sure that my race is not the problem.
- I can easily find academic courses and institutions which give attention only to people of my race.
- I can expect figurative language and imagery in all of the arts to testify to experiences of my race.
- I can chose blemish cover or bandages in "flesh" color and have them more or less match my skin.
- I can travel alone or with my spouse without expecting embarrassment or hostility in those who deal with us.
- I have no difficulty finding neighborhoods where people approve of our household.
- My children are given texts and classes which implicitly support our kind of family unit and do not turn them against my choice of domestic partnership.
- I will feel welcomed and "normal" in the usual walks of public life, institutional and social.
Elusive and Fugitive
I repeatedly forgot each of the realizations on this list until I wrote it down. For me white privilege has turned out to be an elusive and fugitive subject. The pressure to avoid it is great, for in facing it I must give up the myth of meritocracy. If these things are true, this is not such a free country; one's life is not what one makes it; many doors open for certain people through no virtues of their own.
In unpacking this invisible knapsack of white privilege, I have listed conditions of daily experience that I once took for granted. Nor did I think of any of these perquisites as bad for the holder. I now think that we need a more finely differentiated taxonomy of privilege, for some of these varieties are only what one would want for everyone in a just society, and others give license to be ignorant, oblivious, arrogant, and destructive.
I see a pattern running through the matrix of white privilege, a pattern of assumptions that were passed on to me as a white person. There was one main piece of cultural turf; it was my own turn, and I was among those who could control the turf. My skin color was an asset for any move I was educated to want to make. I could think of myself as belonging in major ways and of making social systems work for me. I could freely disparage, fear, neglect, or be oblivious to anything outside of the dominant cultural forms. Being of the main culture, I could also criticize it fairly freely.
In proportion as my racial group was being made confident, comfortable, and oblivious, other groups were likely being made unconfident, uncomfortable, and alienated. Whiteness protected me from many kinds of hostility, distress, and violence, which I was being subtly trained to visit, in turn, upon people of color.
For this reason, the word "privilege" now seems to me misleading. We usually think of privilege as being a favored state, whether earned or conferred by birth or luck. Yet some of the conditions I have described here work systematically to over empower certain groups. Such privilege simply confers dominance because of one's race or sex.
Earned Strength, Unearned Power
I want, then, to distinguish between earned strength and unearned power conferred privilege can look like strength when it is in fact permission to escape or to dominate. But not all of the privileges on my list are inevitably damaging. Some, like the expectation that neighbors will be decent to you, or that your race will not count against you in court, should be the norm in a just society. Others, like the privilege to ignore less powerful people, distort the humanity of the holders as well as the ignored groups.
We might at least start by distinguishing between positive advantages, which we can work to spread, and negative types of advantage, which unless rejected will always reinforce our present hierarchies. For example, the feeling that one belongs within the human circle, as Native Americans say, should not be seen as privilege for a few. Ideally it is an unearned entitlement. At present, since only a few have it, it is an unearned advantage for them. This paper results from a process of coming to see that some of the power that I originally say as attendant on being a human being in the United States consisted in unearned advantage and conferred dominance.
I have met very few men who truly distressed about systemic, unearned male advantage and conferred dominance. And so one question for me and others like me is whether we will be like them, or whether we will get truly distressed, even outraged, about unearned race advantage and conferred dominance, and, if so, what we will do to lessen them. In any case, we need to do more work in identifying how they actually affect our daily lives. Many, perhaps most, of our white students in the United States think that racism doesn't affect them because they are not people of color; they do not see "whiteness" as a racial identity. In addition, since race and sex are not the only advantaging systems at work, we need similarly to examine the daily experience of having age advantage, or ethnic advantage, or physical ability, or advantage related to nationality, religion, or sexual orientation.
Difficulties and angers surrounding the task of finding parallels are many. Since racism, sexism, and heterosexism are not the same, the advantages associated with them should not be seen as the same. In addition, it is hard to disentangle aspects of unearned advantage that rest more on social class, economic class, race, religion, sex, and ethnic identity that on other factors. Still, all of the oppressions are interlocking, as the members of the Combahee River Collective pointed out in their "Black Feminist Statement" of 1977.
One factor seems clear about all of the interlocking oppressions. They take both active forms, which we can see, and embedded forms, which as a member of the dominant groups one is taught not to see. In my class and place, I did not see myself as a racist because I was taught to recognize racism only in individual acts of meanness by members of my group, never in invisible systems conferring unsought racial dominance on my group from birth.
Disapproving of the system won't be enough to change them. I was taught to think that racism could end if white individuals changed their attitude. But a "white" skin in the United States opens many doors for whites whether or not we approve of the way dominance has been conferred on us. Individual acts can palliate but cannot end, these problems.
To redesign social systems we need first to acknowledge their colossal unseen dimensions. The silences and denials surrounding privilege are the key political surrounding privilege are the key political tool here. They keep the thinking about equality or equity incomplete, protecting unearned advantage and conferred dominance by making these subject taboo. Most talk by whites about equal opportunity seems to me now to be about equal opportunity to try to get into a position of dominance while denying that systems of dominance exist.
It seems to me that obliviousness about white advantage, like obliviousness about male advantage, is kept strongly enculturated in the United States so as to maintain the myth of meritocracy, the myth that democratic choice is equally available to all. Keeping most people unaware that freedom of confident action is there for just a small number of people props up those in power and serves to keep power in the hands of the same groups that have most of it already.
Although systemic change takes many decades, there are pressing questions for me and, I imagine, for some others like me if we raise our daily consciousness on the perquisites of being light-skinned. What will we do with such knowledge? As we know from watching men, it is an open question whether we will choose to use unearned advantage, and whether we will use any of our arbitrarily awarded power to try to reconstruct power systems on a broader base.
Peggy McIntosh is associate director of the Wellesley Collage Center for Research on Women. This essay is excerpted from Working Paper 189. "White Privilege and Male Privilege: A Personal Account of Coming To See Correspondences through Work in Women's Studies" (1988).

Korff, J. (n.d.). Welcome to country and acknowledgement of country. Retrieved February 4, 2022 from
Welcome to Country and Acknowledgement of Country are important Aboriginal ceremonies. But what are the differences, who can provide one, and which words should you use?
Aboriginal Protocols of Respect
If you participated in an activity that involved Aboriginal people you might have experienced a Welcome to Country or Acknowledgement of Country.
Both are protocols that precede the activity. They recognise the unique position of Aboriginal people in Australian culture and history and show respect for Aboriginal people. Traditionally, a Welcome to Country was an invitation or permission for a person from a different area to pass through or enter. Doing so without it was unacceptable.
Both ceremonies also acknowledge the land as a living entity – one reason why 'Country' is often capitalised.
Why is a Welcome or Acknowledgement Important?
Incorporating a Welcome or Acknowledgement protocol into official meetings and events shows that you recognise Aboriginal people as the First Australians and custodians of their land. It demonstrates that you, or your organisation, are aware of the past and ongoing connection of Aboriginal people to place and land.
In a business context it shows your organisation's commitment to inclusion and diversity for staff and sends a strong message to future (Aboriginal) applicants. [2]
Unlike New Zealand, Canada and the United States, Australia has no treaty with its Aboriginal people.
A Welcome to, or Acknowledgement of, Country doesn’t replace a treaty, native title or land rights, but they are a small gesture of recognition of the association with land and place of Aboriginal people and their history.
If you are planning to include a Welcome to Country, or do an Acknowledgement of Country, make sure to consult with Aboriginal people of the community where the event takes place. This way you ensure that the ceremony pays the appropriate level of recognition and involves the right people.
Acknowledgements of country and traditional owners are something that decent non-Indigenous people give, not because they feel pushed into it but because they believe it is the right thing to do.
— Koori Mail editorial [3]
Acknowledgement of Country
An 'Acknowledgement of Country' is a way where any person can show awareness and respect for Aboriginal culture and heritage and the ongoing relationship the traditional custodians have with their land. [4]
Both Aboriginal and non-Aboriginal people can perform 'Acknowledgement of Country'. It is a demonstration of respect dedicated to the traditional custodians of the land (or sea) where the event, meeting, school function or conference takes place. It can be formal or informal.
Note that an acknowledgement does not mean you're asking for permission to be on Aboriginal land. For that you'll have to contact an Aboriginal Land Council.
More and more publications permanently include an Acknowledgement, for example the Australian Book Review. [5]
Tips for an Acknowledgement of Country
Below I have compiled a selection of examples from which you can choose a text that suits your needs. Here are some tips for the wording of an Acknowledgement of Country:
- 'Custodians' or 'owners'? Both terms are in use. 'Custodians' reminds of the ongoing obligation to look after country, and that Aboriginal people don't own the land, but it owns them. 'Owner' reminds that their land was never formally ceded to anyone and of Australia's history of denying ownership and Aboriginal people's sovereignty over their lands.
Some Aboriginal organisations refer to 'traditional owners' (TOs) themselves while others dislike the term. A descendant of the Aboriginal people of the Mackay Region told me that he "prefer[s] to be identified as a Traditional Custodian and not a Traditional Owner as I do not own the land but I care for the land." [6] - Include both groups. Always use "Aboriginal and Torres Strait Islanders" to include both distinct First Nations groups.
- Respect Elders. I've capitalised "Elders" as a sign of respect.
- Include land. Always include a reference to Aboriginal land.
- Be personal. I've used “I” rather than the organisation’s name, or "we", to make the acknowledgement more personal. (It's a single person speaking, after all.)
Tip
Using Zoom or Skype? Then your audience is most likely spread across different Aboriginal nations' lands. Ensure to be inclusive, e.g. with "Traditional Owners of the lands we meet on today" and acknowledge "any Aboriginal people joining us today".
Avoid using "emerging leaders" as there is significant discomfort within the Aboriginal community with that term (e.g. who defines the "emerging" leader? Who is a leader?).
Story: The first Acknowledgement
A woman of my subscriber community was surprised and impressed by what happened at an event she was attending:
"Last weekend I went to a family wedding. Of course it was beautiful and special to everyone there.
"The ceremony started with an Acknowledgement of Country. A few of us admitted afterwards that this was the first time we’d experienced an Acknowledgement of Country at a wedding.
"As we were standing outside in a really lovely part of the Southern Highlands in NSW, it was a timely reminder of the traditional owners of the country. Maybe this could become a common part of such important events?"
Spoken, Aboriginal nation known
Replace [Aboriginal group/clan] with the name of the Aboriginal group (e.g. "Gadigal people") and [Aboriginal nation] with the nation's name (e.g. "Eora").
I wish to acknowledge the custodians of this land, the [Aboriginal group/clan] people of the [Aboriginal nation] nation and their Elders past and present. I acknowledge and respect their continuing culture and the contribution they make to the life of this city and this region.
I acknowledge that we are meeting on the traditional country of the [Aboriginal nation] people of the [Aboriginal region] and pay respect to Elders past and present. I recognise and respect their cultural heritage, beliefs and relationship with the land, which continue to be important to the [Aboriginal nation] people living today.
I would like to acknowledge that this meeting is being held on Aboriginal land and recognise the strength, resilience and capacity of [Aboriginal nation] people in this land.
I would like to acknowledge that this meeting is being held on Aboriginal land, the land of the the [Aboriginal group/clan] people of the [Aboriginal nation] nation. I like to pay respect to their Elders past and present.
I would like to acknowledge the [Aboriginal group/clan] people who are the traditional custodians of this land. I would also like to pay my respects to Elders past and present of the [Aboriginal nation] nation, and I extend that respect to other indigenous people who are present.
Before we begin the proceedings, I would like to acknowledge and pay respect to the traditional custodians of the land on which we meet; the [Aboriginal group/clan] people of the [Aboriginal nation] nation.
I am honoured to be on the ancestral lands of the [Aboriginal group/clan] people. I acknowledge the First Australians as the traditional custodians of the continent, whose cultures are among the oldest living cultures in human history. I pay respect to the Elders of the community and extend my recognition to their descendants who are present.
Spoken, Aboriginal nation not known
I acknowledge the traditional custodians of country throughout Australia and recognise their continuing connection to land, waters and community. I pay my respects to them and their cultures; and to Elders both past and present.
I would like to acknowledge the traditional custodians of the land on which we meet today and pay my respects to the Elders past and present. I extend my respect to the Aboriginal or Torres Strait Islander [people/colleagues/staff/students] who are present today.
I acknowledge the traditional custodians of the land we have gathered on today. I pay my respects to the Elders past and present, for they hold the memories, the traditions, the culture and hopes of Aboriginal and Torres Strait Islander peoples across the nation. A better understanding and respect for Aboriginal and Torres Strait Islander cultures develops an enriched appreciation of Australia’s cultural heritage and can lead to reconciliation. This is essential to the maturity of Australia as a nation and fundamental to the development of an Australian identity.
Printed Publications
To include an acknowledgement on a printed document, ideally it should be placed on the inside front cover, standing alone, in a place of significance.
[Organisation] acknowledges the Australian Aboriginal and Torres Strait Islander peoples of this nation. We acknowledge the traditional custodians of the lands on which our company is located and where we conduct our business. We pay our respects to ancestors and Elders, past and present. [Organisation] is committed to honouring Australian Aboriginal and Torres Strait Islander peoples’ unique cultural and spiritual relationships to the land, waters and seas and their rich contribution to society.
Websites and Emails
[Organisation] acknowledges the Australian Aboriginal and Torres Strait Islander peoples as the first inhabitants of the nation and the traditional custodians of the lands where we live, learn and work.
Signs
An increasing number of businesses affix signs to entry areas of their premises. Here's a sample wording:
[Organisation] operates on [Aboriginal nation] country. We acknowledge the [Aboriginal nation] people as the traditional custodians of the [Organisation location] region and pay our respects to [Aboriginal nation] elders past and present. We are committed to a positive future for the Aboriginal community.
Government, organisations and even small groups are adopting the practice of acknowledging the traditional owners.
For more information contact the NSW Aboriginal Education Consultative Group Inc. The Sydney Morning Herald offers a video with a few sample acknowledgements.

Australia Post acknowledges traditional owners with a sign in major retail outlets around Australia. The sign was part of their 2011 Reconciliation Action Plan [7]. The colours represent both Aboriginal and Torres Strait Islanders along with an imprint of a stamp.
Acknowledgement of Country' by Jonathan Hill
Today we stand in footsteps millennia old.
May we acknowledge the traditional owners
whose cultures and customs have nurtured,
and continue to nurture, this land,
since men and women
awoke from the great dream.
We honour the presence of these ancestors
who reside in the imagination of this land
and whose irrepressible spirituality
flows through all creation.
Jonathan Hill is a poet living in New South Wales. [8]
Criticism
Some politicians have voiced concern that the 'Acknowledgement of Country' was an "empty" gesture of political correctness and looked "like tokenism" if it was performed too often [9]. The Victorian Premier decided to scrap a requirement for ministers and departmental staff to acknowledge traditional owners in May 2011 [10].
Government policies which force departments to do 'Acknowledgement of Country' and have 'Welcome to Country' ceremonies performed undermine the genuine gesture and make it "feel false", argues Sue Gordon, a retired West Australian magistrate [9].
The Aboriginal community does not share these views.
David Ross, director of the Central Land Council, feels that one should not ignore the "existence and ownership of this land by Aboriginal people before European settlement" and acknowledge the black history with the ritual. Opposing 'Welcome to Country' ceremonies would encourage racist elements within the community.
"Our own view is that welcomes to and acknowledgements of country—if conducted in a meaningful , genuine and thoughtful way—are the least we should be able to expect from our visitors to our land," say the editors of the Koori Mail [3].
I think it's fantastic [to do Acknowledgement of Country ceremonies], ten years ago we weren't even acknowledged.
— Warren Mundine, Indigenous business leader [9]
[Acknowledgement of Country] says to the world, and more importantly to ourselves, that we accept the fact we are in a place that has a history and story far beyond 220 years. It says to our Aboriginal and Torres Strait Islander fellow Australians that we are all in the future journey of our country together.
— Richard Wynne, Minister for Aboriginal Affairs, Victoria [11]
Welcome to Country
A 'Welcome to Country' is a small ceremony where traditional custodians, usually Elders or a recognised spokesperson, welcome people to their land.
This is a significant recognition and is made through a formal process, although it's up to the Elder how they decide to carry out the ceremony. It also depends on the location of the event and the practice of the Aboriginal community which can vary greatly according to region.
During a 'Welcome to Country' the Elder welcomes those in attendance, guests, staff or students to their Country. It might be just a simple speech or a performance of some sort, like a song, traditional dance, a didgeridoo piece or any combination of these.
'Welcome to Country' should always occur at the opening of the event in question, preferable as the first item. Note that a 'Welcome to Country' is often considered a right and not a privilege.
Protocols for welcoming visitors to country have been a part of Aboriginal culture for thousands of years.
Despite the absence of fences or visible borders, Aboriginal groups had clear boundaries separating their country from that of other groups. Crossing into another group’s country required a request for permission to enter — like gaining a visa — and when that permission was granted the hosting group would welcome the visitors, offering them safe passage [12].
In modern Australia, the 'Welcome to Country' ceremony was first conducted at an official ceremony in 1999 during the NSW Supreme Court's 175th anniversary, arranged by Chief Justice James Spigelman. [13]
In parliament it was first introduced at the start of parliament in 2008 and now forms a regular element of Australian political process. [14]Find a Local Aboriginal Land Council to help you organise a Welcome to Country.
Welcomes [to country]… are what traditional owners give—if they so desire. There should be no expectation or demand for this to be the case.
— Koori Mail [3]
Fact
In 2019, Canberra Airport added a Welcome To Country to its international terminal, spoken in Ngunnawal, the traditional Aboriginal language of the ACT region, and translated to English.
In 2015, Sydney's New Year's Eve fireworks were ushered in for the first time with a huge Aboriginal Welcome to Country ceremony, putting local Gadigal, Wangal and Gamaragal traditions front and centre in the global new year celebrations.
Welcome to Country Can Be Bittersweet
Bev Manton, chairperson of the New South Wales Aboriginal Land Council (NSWALC), explains how giving a Welcome to Country can be bittersweet. [15]
"A Welcome to Country is about Aboriginal people acknowledging the past, and looking to the future. It is often delivered by an Aboriginal person who has themselves been the victim of government policies.
"Our Elders do the Welcome to Country as an act of generosity. These are the same people who have had their children taken away, or been removed themselves. They're the same people who had their wages stolen by successive governments. They're the same people who had ancestors remains raided by grave robbers. They're the same people who were disposed from their lands and forced on to missions and reserves.
"And yet despite all of these terrible events—despite the horrendous treatment by so many parliaments—these very same people are still prepared to say 'welcome' to the very people who in some cases have presided over the oppression."
For Michael Ghillar Anderson, Head of State of the Euahlayi Peoples Republic in northern NSW, a Welcome means allowing too much. [16]
"How serious can one be with a Welcome [to Country], when you are paid to Welcome them to Country? That cannot be serious at all. It’s a money-making venture, a community income stream, without any real substance and meaning, but the invaders take it seriously, even though they pay you.
"Once you welcome them to country, whether you mean it or not, in their world you are opening the door and letting them in and what is your’s becomes their's. Right now their only legitimacy on country is when they are welcomed in."
Charles (Mibunj) Moran, a Bundjalung elder from northern NSW, explains how a Welcome respects past generations: "When we have our Welcome to Country our custodians/Elders pay respect to custodians past and present as well as Elders past and present.
"Spiritually, this is showing respect for the country and the custodians who are responsible for taking care of the country where we live... So what our custodians are doing is trying to give respect back into the country." [17]
I have come to learn that the Welcome to Country ceremony is such an important aspect of Indigenous Australia… They're unique and special and, in essence, a respectful gesture from the traditional peoples to all people, visitors and friends.
— Matiu Paki, a Maori from the North Island of New Zealand [18]
Story: Traditional welcome: Entering country the proper way
Read how a Ngarinyin tribal elder explained a traditional welcome to country [19]: "Before whitefellas came, it was the tradition of Aboriginals that when strangers came into their particular country to hunt or to gather, or to just pass through on their way to other places, that the host Aboriginals would go out to welcome them.
When they met, there would be the formalities of greeting. Part of the ceremony of welcome would be the men sitting around and talking men’s business whilst the host women would take the visiting women and children to a women’s site to talk women’s business.
When this was completed, the two groups would join again and the men would hunt for kangaroo, goannas or bush turkey - and the women would prepare an area for eating and would gather firewood and berries, fruit, nuts and lily roots for a meal.
Then the ceremonies—the corroborees or jumbas would commence—and the dancing, the singing around the fire could well go on, not only all night, but sometimes for many nights in a row. Each jumba with a message—each with its own story—men, women and children taking part. Whilst during the day, the visiting tribe would be taken and shown the sites of significance and be told the stories of the spirit of the land they would be passing,
In this way, the hosts believed that by the end of formalities, when the strangers were ready to move on - they would not be considered strangers but friends who now had the spirit of the country in their hearts—they carried the Wunggud with them—just like the people who lived there.
They believed that once the spirit of the land was in their hearts, then those people would never damage the land - they would love it and care for it like those whose home country it was..."
Can a Welcome or Acknowledgement Help Aboriginal People?
Aboriginal people are disadvantaged in many areas of their life as statistics show.
But what can be done, alongside efforts in health, education and employment, are practices of inclusion. Including recognition of Aboriginal people in events, meetings and national symbols shows your respect, and respect is a good base on which Aboriginal and non-Aboriginal Australians can come closer and eventually reconcile.
Haven't Aboriginal people lost their land?
All areas of Australia have or had traditional owners, including where there are now large cities.
Even though Aboriginal people may not live in a traditional way on this land, they are still connected to it.
In Aboriginal culture, the meaning of country is more than just ownership or connection to land, as Aboriginal Professor Mick Dodson explains:
"When we talk about traditional ‘country’... we mean something beyond the dictionary definition of the word. For Aboriginal Australians...we might mean homeland, or tribal or clan area and we might mean more than just a place on the map. For us, country is a word for all the values, places, resources, stories and cultural obligations associated with that area and its features. It describes the entirety of our ancestral domains." [12]
Story: Welcoming babies to country
Across Australia, Aboriginal families are reviving the tradition of welcoming new babies to country.
They smear the baby's face with ochre, fit a headband made by aunties, and gift them an animal skin, similar to one that would have been used generations ago to wrap newborns. [20]
The purpose of this ceremony is to kick-start a cultural understanding for their children, to start a sense of identity which was denied to many Aboriginal people. Culture protects families and individuals and, so the hope, can reduce the number of children who are removed from their families, a government practice that continues today.
The ceremony has the support of First 1000 Days Australia, a movement that aims to strengthen Aboriginal families so they can support their children from pregnancy to two years of age in health and wellbeing.
Further Resources
Reconciliation Australia has put together a Frequently Asked Question (FAQ) section on Welcome to Country and Acknowledgement of Country ceremonies.

Prince-Robertson, R., & McDonald, M. (2011). Working with Indigenous children, families, and communities: Lessons from practice. Melbourne, VIC: Communities and Families Clearinghouse Australia. https://aifs.gov.au/cfca/publications/working-indigenous-children-families-and-communities
Planning and delivering services to Aboriginal and Torres Strait Islander children, families, and communities can be a complex task for practitioners and policy-makers. Social problems are often deeply entrenched, and need to be approached with consideration of historical, social, community, family and individual factors. Furthermore, as Australian Indigenous cultures are not homogenous, Indigenous communities can differ considerably. Indigenous communities often have characteristics specific to geographic location, with significant variation evident across urban, rural, and remote communities (Neckowaya, Brownleea, & Castellana, n.d.).
Methods that child and family services can use to support Indigenous families and communities include:
- Working with (rather than working “on”) Indigenous communities;
- Ensuring your service is culturally competent;
- Focusing on attracting and retaining the right staff;
- Cultivating networks and relationships; and
- Adopting an action research approach.
Many Indigenous families and communities in contemporary Australia face immense challenges. Their strength and resilience is compromised by multiple complex problems, including historical and ongoing dispossession, marginalisation, and racism, as well as the legacy of past policies of forced removal and cultural assimilation (Human Rights and Equal Opportunity Commission, 1997). These issues contribute to the high levels of poverty, unemployment, violence, and substance abuse seen in many Indigenous communities. They also impact negatively on Indigenous children, who demonstrate poor health, educational, and social outcomes when compared to non-Indigenous children (Australian Institute of Health and Welfare [AIHW], 2009).
Additionally, there is a number of factors that inhibit the successful delivery of services to Indigenous families and communities. A lack of appropriate infrastructure can hinder the logistics of service delivery. Demanding workloads and low remuneration make staff burnout a common issue. Difficult social environments—with low levels of trust, participation, social control, and efficacy, and high levels of anxiety, disempowerment, disorganisation, and mobility—provide the context for much service delivery. Finally, evidence regarding effective responses to problems in Indigenous communities is limited (Scougall, 2008).
Despite the complexity of these issues, there are services that are working effectively to reduce Indigenous disadvantage in Australia (Flaxman, Muir, & Oprea, 2009; Scougall, 2008). The lessons learnt from these services about what works are critical to ensuring improved outcomes for Indigenous children, families and communities. The impetus to deliver improved outcomes for Indigenous children, families and communities is strengthened by the Council of Australian Governments’ (COAG) Indigenous reform agenda (2010), referred to as “Closing the Gap”. This reform agenda aims to “close the gap” on Indigenous disadvantage across 6 key areas— life expectency, child mortality, access to early childhood education, literacy and numeracy, education attainment, and economic partcipation (COAG, 2010).
This Practice Sheet summarises those lessons and is likely to be of most use to organisations, services, agencies and program/project managers who are planning or delivering Indigenous-specific services, or who are operating in areas where there are large numbers of Indigenous service users.
For more information about research evidence on what works to close the gap on Indigenous disadvantage, visit the Closing the Gap clearinghouse.
Practice Considerations
Practice considerations are general principles based upon lessons from research and practice designed to provide additional guidance to service providers about specific issues relating to children and families, especially as they relate to disadvantaged Australian communities. The following practice considerations are elaborated upon using case studies.
What methods can child and family services use to support Indigenous families and communities?
Work with Indigenous Communities
I approached the Elders and involved them … And they become part of it and they’d say, “We’d like to sit on your advisory [board]”. And in the Aboriginal community, if we’re doing a good job, then everybody knows about it. (Indigenous service provider, as cited in Higgins & Butler, 2007, p. 11)
In the past, some service providers have been criticised for not involving the community in service delivery. Services for Indigenous Australians are most effective when the community is involved in both their planning and implementation stages. When Indigenous Elders, community members, and other local service providers are engaged in a consultative process, the most important needs of the community can be distinguished and the most appropriate methods of implementation can be identified.
Working with (rather than working “on”) Indigenous communities can be achieved when service providers adopt the following principles:
- Involve community members. This includes involvement in both planning and implementation of the service.
- Identify pressing needs. It is important to communicate with community members in order to identify their most pressing needs. Experience suggests that it is often best to start with small and achievable objectives, rather than trying to take on too much too early. Early successes often have a “ripple” effect, inspiring community confidence and motivating service staff.
- Utilise existing networks, services, and resources. Some Indigenous projects have very successfully “piggybacked” services on the back of existing activities, social events, and structures.
- Balance the talking with the doing. In the past, too much community consultation and a subsequent failure to follow through with action has, understandably, led to cynicism among some Indigenous communities. It is important to balance consultation with implementation. This can be effectively achieved if an action research approach is adopted (see the “Adopt an action research approach” section in this paper).
For more information on working with Indigenous communities see: Scougall (2008, pp. 66–67) and Higgins (2004).
Ensure that your service is culturally competent
When I was 9, I was in a really bad place. Experiencing all that I had, I felt like I had lost my soul. I still remember the day I arrived at the agency, it was a lot for me ‘cause I had only had some bad experiences with white fellas before. But there was a Koorie Flag on the wall and a plaque saying your office was on Wurrundjeri land and even though I’m Yorta Yorta I thought maybe, just maybe, it would be different. (Indigenous service user, as cited in Victorian Aboriginal Child Care Agency, 2008, p. 52)
Indigenous Australians have maintained cultures that are in many ways distinct from that of mainstream, non-Indigenous Australia. This cultural difference has implications for both policy and practice. If services do not adapt to the contemporary Indigenous cultural context, they have little chance of improving outcomes in the long term. To be culturally competent, service organisations need to ensure that cultural knowledge shapes (1) the structure of the service; (2) the specific practices and strategies employed; and (3) the selection, training, and actions of individual staff members (as discussed in the section “Focus on attracting and retaining the right staff”).
The following tips on culturally competent service structure and culturally competent practices and strategies will help ensure cultural competence.
Culturally competent service structure
- Deliver services in a creative and flexible manner in response to the changing needs of the community. This includes flexibility not only in the ways that services are provided, but also where they take place.
- Involve Indigenous community members in the planning of the service structure.
- Conduct programs in informal, non-threatening settings such as in a person’s home (even if only initially).
- Ensure that costs to service users are kept to a minimum.
Culturally competent practices and strategies
- Conduct services “in language” (the first language of local people) or, failing this, have translators or people who can present information in plain, accessible English. It is also important to ensure that any metaphors or examples used take account of Indigenous world views and experiences.
- Involve cultural artefacts in services and everyday activities (e.g., traditional Indigenous tools, foods, and artwork).
- Consult and involve family, extended kin networks, and community members in service delivery.
- Invite Indigenous Elders to participate in the program delivery.
For more information on Indigenous cultural competence see Flaxman et al. (2009, pp. 23–28) and the Victorian Aboriginal Child Care Agency (2008).
Focus on attracting and retaining the right staff
What makes it work is people. The staff have expectations of themselves and of colleagues. They’re self-managing. The quality assurance [of the program] comes from the staff. (Indigenous service provider, as cited in Higgins & Butler, 2007, p. 13)
Competent and capable staff members are key to the success of any social service delivery. This is especially true for Indigenous-specific services, where success is often largely dependent on cultural competence and the development of trusting relationships with the community. A strong team in an Indigenous-specific service will have staff who have the following characteristics:
- Strong relationships with Indigenous program participants. This will often be achieved by employing local people as part of a team, who bring with them a deep understanding of cultural issues and a respect for local protocols.
- Personal qualities necessary to work cross-culturally. The ability to carry out “cultural translation” is particularly important. It is necessary that staff members are able to communicate effectively with and between both external stakeholders and program participants.
- Demonstrated skills to do the job. Many projects require people with specific qualifications or expertise in areas such as childhood development, counselling, capacity building, and leadership development.
For more information on attracting and retaining the right staff when working with Indigenous communities see Scougall (2008, pp. 53–55) and Flaxman et al. (2009, pp. 28–30).
Cultivate networks and relationships
Working in partnership with a wide range of local services has been integral to the success of the Project. (Indigenous Project Progress Report, as cited in Scougall, 2008, p. 62).
Research strongly suggests that services working in isolation often struggle to meet the complex needs of vulnerable and at-risk families (e.g., Indigenous families). Services that form partnerships and collaborations with other local community and government organisations are better able to ensure that those in need receive the right assistance. Some examples of organisations with which Indigenous-specific services have collaborated are:
- Government departments and organisations (e.g., housing services, family services, Centrelink);
- Other local service providers, both mainstream and Indigenous-specific (e.g., drug and alcohol services, community counselling services);
- Health care providers (e.g., health care and sexual health clinics, mental health services);
- Indigenous cultural centres and organisations;
- Schools, TAFE institutions, and universities;
- Child care centres, parenting education providers, and toy libraries; and
- Local businesses and shops.
For more information on collaboration with Indigenous-specific services see Scougall (2008, pp. 60–62) and Soriano, Clark, and Wise (2008).
Adopt an action research approach
Our critical community of action researchers working together, reflecting, sharing, and thinking includes the Yolngu elders, the Yolngu action group, Balanda [non-Indigenous] teachers, and a Balanda researcher to help with the process. Of course, she [the researcher] is involved too; she cares about our problems, she has a stake in finding solutions—this too is different from the traditional role of a researcher. (Mandawuy Yunupingu, then head of the Yirrkala Ganma Education Project, as cited in Denzin & Lincoln, 2005, p. 584)
Action research is a participatory group process aimed at continual evaluation and improvement of practice. It helps to tailor projects to local environments and situations. An action research approach may be useful to services during the planning phase of a program. It has been noted that there is compatibility between action research methods and traditional Indigenous cultural practices and ways of working. Action research involves a dynamic and cyclical process of planning, acting, observing, and reflecting:
- Planning: team members and interested parties come together to define the problems they are facing and to identify the most appropriate ways to tackle these problems;
- Acting: the team proceeds with their planned activity or program of activities;
- Observing: the team observes the operation of the program, gathering information and seeking feedback from all involved;
- Reflection: team members reflect on their observations, and identify areas where there is room for improvement; and
- Planning: the cycle begins again, taking account of what has already been learned.
For more information on the action research approach, see Scougall (2008, pp. 62–65) and Lienert (2002a, 2002b).
Working with Indigenous families: Practice examples
There are many examples within CAFCA’s Promising Practice Profile database of promising and innovative methods that have been used by services and programs to support Indigenous families and communities.
For example, one program delivers locally inclusive and culturally respectful pregnancy and parenting education for young people, especially those in rural and remote Indigenous communities. The program was developed in response to community and school-based requests. Community members are involved in each step of the planning and administration of the program. This involves:
- Extensive preliminary promotion, liaison, and networking with key community members: including Indigenous Elders and members of the community health sector, the educational sector, appropriate government departments, women’s centres, youth services, and local community stores;
- Comprehensive needs analysis: to guarantee that the program meets the unique needs of individual communities;
- Fluidity and flexibility around training approach and timing: so that activities do not conflict with local community customs (e.g., inappropriate site selection) and events (e.g., festivals, funerals); and
- Discussion, negotiation, and careful consideration of program content and manner of delivery: to ensure that activities incorporate traditional/cultural practices and address any language or literacy needs.
Another service, an early intervention program for at-risk young people between the ages of 12 and 17, consists of intensive weekend camps and follow-up support groups; 30% of their clients are Indigenous. At the camps, young people can talk through issues that are affecting their lives and learn how to more effectively handle them. The Program’s innovative staff structure includes three key roles:
- Youth leaders. The leaders facilitate most of the sessions. Youth leaders are people aged 12 to 17 years who have been through three or more camps themselves, who have made positive changes in their lives, and who are dedicated to living by a Youth Insearch Code of Ethics. It has been found that youth leaders are often powerful, credible role models for program participants. It can be a transformative experience for disenfranchised Indigenous youths to see their peers taking steps to improve their own lives.
- Youth liaisons. These are full-time employees with a diploma or degree in Youth Work and/or Community Services. They organise and support the youth leaders.
- Indigenous volunteers. Indigenous volunteers assist in creating a trusting environment for Indigenous youth leaders and camp participants, and help to interpret culturally sensitive issues. They are part of a wider group of volunteers who work together to support the youth leaders in conducting camps.
For a full list of Promising Practice Profiles relating to Indigenous families and communities,
See: www.aifs.gov.au/cafca/topics/targetgroup/targetgroup.html#indigenous.

SNAICC – National Voice for our Children. (2020). Creating change through partnerships: An introductory guide to partnerships between Aboriginal and Torres Strait Islander and non-Indigenous organisations in child and family services.
Introduction
Aboriginal and Torres Strait Islander families and communities have unique richness, diversity and strengths in child rearing. The majority of Aboriginal and Torres Strait Islander families are strong, resilient and nurturing and provide supportive, loving and positive environments for children.
However, some families and communities also continue to face significant challenges in overcoming the impacts of colonisation, including historic and ongoing discrimination and exclusion, systemic child removal, intergenerational trauma, dislocation from land and culture, community disempowerment and poverty. Members of the Stolen Generations and their descendants – who comprise an estimated 33% of the Aboriginal and Torres Strait Islander adult population – still experience adverse outcomes across a broad range of health, socioeconomic and cultural indicators (AIHW, 2019).
Data across areas of family safety and wellbeing and early childhood development show that some families are in need of additional support. While most Aboriginal and Torres Strait Islander children start school on track for a positive educational experience, a significant minority begin at a disadvantage. Aboriginal and Torres Strait Islander children are 2.5 times more likely than non-Indigenous children to be developmentally vulnerable on two or more domains at the time they start school (AEDC, 2018) and are now 10.2 times more likely to be in out-of-home care then non-Indigenous children (SNAICC, 2019).
Engagement with child and family support services is critical to strengthening Aboriginal and Torres Strait Islander families and improving life outcomes for vulnerable children. Statistics indicate a low national level of access to support services by Aboriginal and Torres Strait Islander families, and support services regularly identify Aboriginal and Torres Strait Islander families as ‘hard-to-reach’ (Family Matters, 2019). However, this is more properly characterised as a service system that presents significant barriers to Aboriginal and Torres Strait Islander engagement; barriers that can be overcome by service adaptation and quality service provision (Ware, 2012).
Two key means to increase access to and engagement with children and family services for Aboriginal and Torres Strait peoples are for services to be:
- Working within a cultural competence framework
- Engaging in effective partnerships with Aboriginal and Torres Strait Islander communities and organisations. (SNAICC, 2012).
Based on all available evidence, genuine and respectful partnerships between Aboriginal and Torres Strait Islander community-controlled organisations and non-Indigenous service providers have multiple benefits, including:
- Ongoing cultural competence and safety capability development for non-Indigenous service providers
- Governance and service capacity development for Aboriginal and Torres Strait Islander organisations
- Development of shared capacity to respond to community needs
- Development of individual and community capacity for Aboriginal and Torres Strait Islander peoples in areas including workforce and community leadership.
These benefits are consistent with national and state and territory government policy frameworks that acknowledge the need for, and support, a partnership-based approach with Aboriginal and Torres Strait Islander communities and organisations for service delivery.
However, while partnerships have long been recognised as important for developing effective and culturally competent and safe services, many Aboriginal and Torres Strait Islander people have had negative experiences of tokenistic relationships labelled as partnerships. This has led to a level of mistrust of governments and non-Indigenous services and a belief that they may use partnerships to ‘tick boxes’ of cultural competence and community engagement, without a deeper commitment to sustainable relationships or local community empowerment.
Tokenistic involvement of Aboriginal and Torres Strait Islander people doesn’t lead to better services for Aboriginal and Torres Strait Islander families. It can, in fact, hold up progress, as the appearance of partnership masks deeper mistrust, maintains power imbalance and fails to promote reconciliation. Achieving better outcomes requires a shared commitment to building deeper, respectful and more genuine relationships.
SNAICC has developed this resource with the aims of:
- Introducing organisations to the importance of genuine inter-agency partnerships between Aboriginal and Torres Strait Islander and nonIndigenous service providers.
- Providing an overview of the principles and practices that are effective to create and sustain genuine inter-agency partnerships.
- Introducing service providers to the range of best practice materials available to support services in genuine partnership development.
Partnerships and Self-Determination
Genuine partnerships between Aboriginal and Torres Strait Islander organisations and non-Indigenous service providers are important because they can support the creation of an environment in which Aboriginal and Torres Strait Islander peoples and communities can work towards self-determination – the collective right of peoples to determine and control their own destiny. The Bringing Them Home report explained self-determination in the following way:
Self-determination requires more than consultation because consultation alone does not confer any decision-making authority or control over outcomes. Self-determination also requires more than participation in service delivery because in a participation model the nature of the service and the ways in which the service is provided have not been determined by Indigenous peoples. Inherent in the right of self-determination is Indigenous decisionmaking carried through into implementation (Commonwealth of Australia, 1997).
Community Control Leading to Better Outcomes
International and Australian evidence strongly supports the importance of Indigenous participation for achieving positive outcomes in service delivery for Indigenous children and families.
Canadian research has shown a direct correlation between increased Indigenous community-control of services and improved health outcomes for Indigenous peoples (Lavoie, J. et. al., 2010) and a direct connection between Indigenous selfgovernment and reduced rates of youth suicide (Chandler, M. and Lalonde, C., 1998). Numerous Australian reports and inquiries confirm a lack of robust community governance and meaningful Indigenous community participation as major contributors to past failures of government policy, and commonly highlight the importance of building capacity for Aboriginal and Torres Strait Islander community-controlled children and family services (ANAO, 2012; NSW Ombudsman, 2011; Wild, R. and Anderson P., 2007).
Partnerships that support self-determination extend beyond consultation to provide the resources that genuinely give power to Aboriginal and Torres Strait Islander communities to design and implement policy and programs and to make the decisions about children’s development and wellbeing.
Enabling and respecting self-determination means that partnership cannot be imposed on an Aboriginal and Torres Strait Islander community or organisation; it needs to be based on the aspirations and interests of that community to engage in partnerships and service delivery. One of the key outcomes of any partnership should be, where required and wanted, to build the operational and leadership capacity of the Aboriginal or Torres Strait Islander entity, in line with the aspirations of that entity for increasing its role and service offering for families. It also requires recognising the existing strengths of Aboriginal and Torres Strait Islander people and organisations, including that in many cases a partnership to ‘build capacity’ may not be wanted or required when an organisation already has significant capability and is already best placed to lead service provision for Aboriginal and Torres Strait Islander families.
Key Considerations for Aboriginal and Torres Strait Islander Organisations
Aboriginal and Torres Strait Islander organisations need to consider the value of a potential partnership for meeting the needs of children and families in their community and for advancing their own service development aspirations. It is important that Aboriginal and Torres Strait Islander organisations undertake due diligence to ensure that any potential partnership will benefit you and your community.
Some key questions for consideration by Aboriginal and Torres Strait Islander organisations prior to engaging in partnerships include:
- What services do we want to develop and provide and do prospective partners have the right skills and expertise to support us in developing those services?
- Are prospective partners committed to working respectfully in ways that are culturally safe for our organisations, and for our community?
- Do prospective partners have the capacity to question Western knowledge and privilege Aboriginal and Torres Strait Islander cultural knowledge in their work with Aboriginal and Torres Strait Islander families?
- Are there other Aboriginal and Torres Strait Islander organisations we could partner with to support our service goals rather than partnering with a non-Indigenous provider?
- Will the partnership lead to better supports and outcomes for children and families?
- Are there services we don’t currently deliver and/or don’t want to deliver that we need to partner on to ensure families in our community have access to necessary supports?
- Do prospective partners share our commitment to building capacity, skills and leadership in the local Aboriginal and Torres Strait Islander community?
- Are we best placed to be the lead partner in a program or service for our community, and if not, is that something we want to change as our capacity develops over time?
Answering these questions is an important step to inform whether and how an Aboriginal and Torres Strait Islander organisation negotiates to establish any partnership to deliver services for children and families in your community.
Partnership Principles
SNAICC has identified through research with promising partnerships across Australia (SNAICC, 2012), that the core principles that underpin genuine and successful partnerships between Aboriginal and Torres Strait Islander organisations and non-Indigenous service providers are:
| Principle | This requires.... |
|---|---|
| Commitment to long-term sustainable relationships based on trust | Significant time spent building relationships between staff, organisations and community. Partners commit to ongoing relationship, not only an activity or project. |
| Respect for Aboriginal and Torres Strait Islander cultures and history | Commitment to build cultural understanding, to consult and listen to the local community, and to value Aboriginal and Torres Strait Islander knowledge and professionalism. |
| Commitment to selfdetermination for Aboriginal and Torres Strait Islander peoples | Empowering Aboriginal and Torres Strait Islander communities to lead the response to child and family needs. Building Aboriginal and Torres Strait Islander community, organisation and workforce capacity. |
| Aim to improve long-term wellbeing for Aboriginal and Torres Strait Islander children, families and communities | Identifying and sharing respective strengths in supporting children and families. Partnership resources viewed as community resources and shared for the benefit of children and families. |
| Shared responsibility and accountability for shared objectives and activities | Negotiated and shared vision is developed. Partners jointly develop indicators of success and work together to monitor and evaluate progress. |
| Valuing process elements as integral to support and enable partnership | Agreements clarify commitments, roles and accountability. Time and resources are allocated to joint planning, review, and partnership development. |
| Redressing unequal or discriminatory relationships, structures and outcomes | Recognising that Aboriginal and Torres Strait Islander disadvantage reflects historical and continuing discrimination, and working to correct resulting power and resource imbalances. |
| Working differently with Aboriginal and Torres Strait Islander children and families | Developing cultural competence and safety in service delivery. Recognising non-Indigenous approaches are often not the best way to engage and support Indigenous families. |
These principles form the bedrock of genuine and successful partnerships, and have major implications for partnership development, operation, management and resourcing.
Overview Of How to Create And Sustain Genuine Inter-Agency Partnerships
The framework below provides a way of understanding and thinking about partnership development. It draws on the evidence of what is important for genuine partnerships in service delivery for Aboriginal and Torres Strait Islander children and families. The outer boxes describe the four key domains that inform all the processes that take place in the inner-circle with the aim to achieve the core objective at the centre of the diagram [on the next section].
Key Strategies
The four key strategies outlined below expand further on how you can use this framework to build and maintain genuine partnership.
Strategy 1: Build Your and Your Organisation’s Cultural Competence
In genuine partnerships, non-Indigenous organisations have a responsibility to develop culturally competent and safe professional practice. Cultural competence forms the basis of an organisation’s readiness to engage respectfully with Aboriginal and Torres Strait Islander people and organisations. Delivering culturally safe services requires ongoing learning and commitment, particularly for non-Indigenous organisations. In a partnership, Aboriginal and Torres Strait Islander organisations and people can often take roles in sharing and teaching about their cultures and supporting others to develop their knowledge and understanding, but these roles need to be valued and resourced within a partnership.
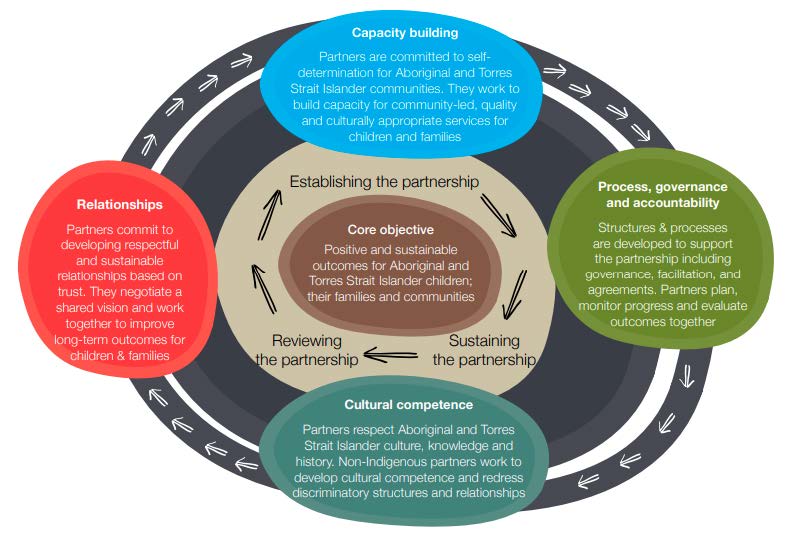
One of the key outcomes of a partnership should be to build the cultural capability and safety of non-Indigenous parties. All service providers have a responsibility to respect and protect the internationally recognised rights of children and all Indigenous peoples to maintain and practice their cultures (UNCRC, article 30; UNDRIP, article 11). Research demonstrates that cultural competence is important for all services to better engage with and support Aboriginal and Torres Strait Islander families, and that family support services are most impactful when programs incorporate cultural knowledge and are focused on the strengths of Aboriginal and Torres Strait Islander families (AIFS, 2012). However, it must always be remembered that no one can become fully competent in a culture that is not their own, and that developing cultural capability does not serve as a substitute for enabling and supporting the genuine cultural authority of Aboriginal and Torres Strait Islander people and organisations.
There are a number of resources that nonIndigenous organisations and governments can refer to when starting their cultural competence learning (see the Further resources section below). Keep in mind that while you can begin by reading and learning more, genuine cultural competence is not something that can be learnt from a book. Cultural competence develops primarily through relationships with Aboriginal and Torres Strait Islander people and communities.
REMEMBER: Developing cultural competence is a continuous learning journey, not a destination. It requires a change in attitudes and practices through which individuals and organisations demonstrate genuine respect and value for a culture that is not their own. The continuum below provides a way to think about a cultural competence journey (VACCA, 2008).

| Cultural Destructiveness | Cultural Incapacity | Cultural Blindness | Cultural Pre-competence | Cultural Competence | Cultural Proficiency |
|---|---|---|---|---|---|
| Intentional attitudes, policies and practices that are destructive to cultures and consequently to individuals within the culture | Lack of capacity to help minority clients or communities die to extremely biased beliefs and a paternal attitude toward those not of a mainstream culture | The belief that service or helping approaches traditionally used by the dominant culture are universally applicable regardless of race or culture. These services ignore cultural strengths and encourage assimilation | The desire to deliver quality services and a commitment to diversity indicated by hiring minority staff, initiating training and recruiting minority members for agency leadership, but lacking information on how to maximise these capacities. This level of competence can lead to tokenism | Acceptance and respect for difference, continuing self assessment, careful attention to the dynamics of difference, continuous expansion of knowledge and resources, and adaptation of services to better meet the needs of diverse population | Holding culture in high esteem; seeking to add to the knowledge based of culturally competent practice conducting research, influencing approaches to care, and improving relations between cultures. Promotes self determination |
|
BUILDING AND MAINTAINING CULTURAL CAPACITY ISN’T ALWAYS EASY Some of the challenges expressed in SNAICC’s 2019 partnership survey1 , by organisations currently in partnerships: |
‘Maintaining our cultural competence to provide effective services to the organisations has been a challenge.’ |
|---|---|
| ‘We are a non-Indigenous organisation that has a history of not respecting the knowledge that comes with local Indigenous groups, and a history of trying to Westernise responses to issues and discounting the ideas and solutions developed by Indigenous community members and organisations. This makes it really important that if we say we will do something, we follow through. Also, we need to be honest if we can’t support something, and say so.’ | |
| ‘Sometimes our work appears tokenistic; not taking the time to get to know the organisation and therefore not having strong relationships has made things challenging.’ |
|
HELPFUL HINTS! Some of the things that have helped partnerships to flourish, expressed in SNAICC’s 2019 partnership survey, by organisations currently in partnerships: |
‘As a non-Indigenous organisation we are aware that we don’t have all of the knowledge and history on our own, and we are genuinely committed to learning from our partners and to continuously improve our services. We maintain a joint commitment to deliver safe, appropriate and family-centred services.’ |
|---|---|
| ‘We have established a set of protocols for staff visiting community, which have been endorsed by a senior cultural advisor in this region. This process of creating protocols for engaging with Aboriginal communities is being implemented across our service footprint through our Reconciliation Action Working Group. Our partnerships have been working well because we have been able to seek guidance from our Aboriginal staff to help non-Aboriginal staff to work respectfully and in a culturally appropriate way.’ | |
| We have a strong commitment to employing playgroup facilitators from community. We work to engage Elders and community leaders to assist in strengthening connections to families. We support the families to connect to culture and traditions through the playgroup experience and we are led by the expertise of the local families and services.’ |
|
WHAT ELSE CAN WE TRY? Useful strategies to build the cultural competence that underpins genuine partnerships include: |
Identify local cultural training provided by Aboriginal and Torres Strait Islander people or organisations and build this into induction and training for staff (your partner organisations may be able to support with this). |
|---|---|
| Develop a cultural capability development plan for your organisation. SNAICC has a tool available for cultural capability planning, that can be found on page 32 of SNAICC’s Partnership Training Manual. | |
| Establish staff sharing and shadowing arrangements with Aboriginal and Torres Strait Islander organisations to create opportunities for cross-cultural learning between staff. | |
| Create a plan for increasing Aboriginal and Torres Strait Islander employment at your organisation, including in senior positions and for supporting the retention and professional development of Aboriginal and Torres Strait Islander staff. |
Reflective Exercise
In reflecting on your cultural competence, consider:
- Have you read the leading cultural competency framework documents?
- Have you learned about Aboriginal and Torres Strait Islander culture, customs, history and language? Which organisations and people have helped you to learn?
- Who could you learn more from? Are there relevant cultural awareness programs you can attend?
- How have you supported and encouraged other people to learn?
- Which stage of the cultural competence continuum do you think you are at?
- Have you developed a cultural competence development plan for your organisation?
Where to From Here?
Leading cultural competence framework documents identified by SNAICC include:
- The SNAICC Working and Walking Together resource, which is designed to support family relationship services to work with Aboriginal and Torres Strait Islander families and communities.
- The VACCA Aboriginal Cultural Competence Framework developed for the Victorian Department of Human Services. This framework is incorporated within agency registration standards for community service organisations providing child and family services and out‐of‐home care services in Victoria. This framework reflects an acknowledgement by the Victorian Government ‘that recognition of Aboriginal self‐determination and the provision of culturally competent services are fundamental to improved outcomes.’
- The VACCA Building Respectful Partnerships resource, which was developed in a partnership between VACCA, Berry Street and MacKillop Family Services. This resource is designed as a practice guide to describe culturally competent and respectful practice across an organisation, with the aim to improve outcomes for Aboriginal children and families and strengthen partnerships between Aboriginal and non-Indigenous organisations.
Strategy 2: Spend Time Building Respectful Relationships of Trust with Aboriginal and Torres Strait Islander People and Communities and Their Organisations
A significant commitment to and investment in developing relationships of trust is necessary to enable genuine and respectful partnerships. This is especially important for non-Indigenous service providers that need to re-establish trust that has been damaged by the history of mistreatment of Aboriginal and Torres Strait Islander peoples.
Below are some key ways for non-Indigenous service providers to establish respectful relationships with Aboriginal and Torres Strait Islander children, families, communities and organisations.
CONNECT
Partnership development takes time, resources and commitment. Take the time to get to know people within the Aboriginal and Torres Strait Islander community, to understand community leadership structures and the role of community organisations, and to listen to Elders.
LISTEN
To Aboriginal and Torres Strait Islander people and communities. Consult with the local Aboriginal and Torres Strait Islander community through their own representative organisations and leadership structures. Listen to the needs that they identify and respond by working with them to provide supports that they request. Be aware of and use common protocols for respectful engagement with Aboriginal or Torres Strait Islander communities.
STICK AROUND
Strong partnerships and the building of trust that underpins them take time to develop. To build the trusting relationships that enable you to work effectively with communities to support their wants and needs, you need to commit to working with them for a sustained period of time. One way that you can signify your intention to engage in long-term collaboration is to create a partnership agreement, such as a Memorandum of Understanding (MOU), which clarifies the partnership objectives and the commitment of all parties.
However, agreements rarely drive the relationship. Their quality reflects the process of relationship building, and the open and honest negotiation that underpins the agreement. Good partners recognise that special attention is needed to incorporate Aboriginal and Torres Strait Islander perspectives in agreements, including recognition from non-Indigenous partners of the important leading role of Aboriginal and Torres Strait Islander organisations in identifying needs, and designing and delivering responses for Aboriginal and Torres Strait Islander children and families.
| Some Tips for Creating a Good MOU |
|---|
| Make sure the MOU is focussed on what the partnership is about. It should be a way to describe what you are doing and why in plain language that everybody can understand. Everyone involved should be able to relate to, refer to and use the MOU to guide the partnership. |
| Make sure that the roles and responsibilities of everyone involved are clearly articulated, including who will take the lead on funding applications. It is also important to establish any training, capacity building or skills transfer that will occur throughout the partnership, and who is responsible. |
| Pay attention to when the agreement will end or be up for renewal. In many partnerships that include Aboriginal and Torres Strait Islander organisations it has been recognised as important to have ‘sunset clauses’ through which the partnership ends and the Aboriginal and Torres Strait Islander organisation takes full control of services for their community. It is also important to agree on a detailed transition plan, including timelines for transition over an extended period to better support the Aboriginal and Torres Strait Islander organisation if required. If complete transition of services is not the intention, it will still be important to think about how roles will change over time. |
| A core component of an MOU is the partnership governance structure or committee. If setup well, this group will be an engine room for driving and oversight of the partnership, and accountability to the community. Pay particular attention to how this is created and described. Does it enable a leading role for Aboriginal and Torres Strait Islander organisation/s and community in the response to community needs? |
| Celebrate the signing of an MOU and hold an event that includes the broader community to inform them about the partnership and build excitement around what it can achieve and contribute to the community |
| Make sure that the agreement includes a clause that states the intention that the agreement will not be legally binding. This will assist to ensure there are no unintended legal consequences of the agreement. However, even though the MOU is stated to be not legally binding, it is advisable to get legal advice. |
| See SNAICC’s Partnership Training Manual for further information on agreement making. |
|
BUILDING RESPECTFUL RELATIONSHIPS OF TRUST TAKES TIME AND WORK Some of the challenges expressed in SNAICC’s 2019 partnership survey1 , by organisations currently in partnerships: |
‘Finding time to develop relationships can be a challenge and is often also a challenge in service delivery. Trust can take significant time to be gained with organisations and community groups. The need to meet targets can overshadow the need for time to develop trusting relationships which are just as important.’ |
|---|---|
| ‘Partnership takes time and this is rarely reflected in funding agreements that are largely output driven. It is important that we take the time to learn about each other and see whether our organisations resonate with each other. For example, do we have the same values and mission? This is critical to establish early on in a partnership.’ | |
| ‘Relationships and understanding is built with time, and at times it is difficult to spend the time you would like to foster the relationship or to have the appropriate availability.’ |
|
HELPFUL HINTS! Some of the things that have helped partnerships to flourish, expressed in SNAICC’s 2019 partnership survey, by organisations currently in partnerships: |
‘The relationships are the most important element. For us, if we rely too much on one person to be the “keeper”; of the relationships, it doesn’t work, so we try to bring others along in a kind of succession process.’ |
|---|---|
| ‘Good communication and engagement with the Elders is really helpful.’ | |
| ‘The ability to share ideas and talk about systemic issues is helping us to improve services.’ | |
| ‘Spending time together, listening to stories and valuing shared ideas and contributions from all has had really positive results.’ |
|
WHAT ELSE CAN WE TRY? Useful strategies to build the cultural competence that underpins genuine partnerships include: |
Build your connections with the Aboriginal and Torres Strait Islander community by speaking with Elders, attending community events, and undertaking shared activities with Aboriginal and Torres Strait Islander organisations. |
|---|---|
| Hold a partnership building session to discuss your values and goals with Aboriginal and Torres Strait Islander partners and to build shared understanding. This will set the basis for establishing partnership agreements and activities. | |
| Create opportunities for staff to interact and share knowledge about best practice for supporting Aboriginal and Torres Strait Islander families. This might be through informal get-togethers, shared planning sessions, or shared training. | |
| Torres Strait Islander peoples and better outcomes for Aboriginal and Torres Strait Islander children and families. Explain to partners and community members what this means to you. |
Reflective Exercise
- Have you read the leading relationship-building documents?
- Have you identified what Aboriginal and Torres Strait Islander organisations in your community work in a similar field to you and that you should connect with?
- How can you develop respectful relationships with your local Aboriginal and Torres Strait Islander community?
- Have you introduced yourself to and spoken with Elders in the community about what their priorities are?
- If you are engaged in a partnership, have you developed a partnership agreement?
Where to From Here?
Leading relationship-building documents identified by SNAICC include:
- SNAICC’s Opening Doors Through Partnerships report, which provides practical steps that Aboriginal and Torres Strait Islander organisations, non-Indigenous service providers and government can take to develop and support genuine partnerships that address Aboriginal and Torres Strait Islander needs. The report profiles case studies of good partnership development from across Australia, including interviews with service providers.
- Australian Institute of Health and Welfare and Australian Institute of Family Studies, Engagement with Indigenous Communities in Key Sectors produced for the Closing the Gap Clearinghouse, which provides an overview of how non-Indigenous organisations can effectively engage with Aboriginal and Torres Strait Islander people and communities.
- SNAICC’s Partnership Training Manual, which provides helpful hints in establishing respectful relationships with Aboriginal and Torres Strait Islander people and communities.
Strategy 3: Listen and Learn from Aboriginal and Torres Strait Islander Peoples to Determine How You Can Support Capacity for Community-Led Responses
Non-Indigenous organisations need to listen to the needs and aspirations of Aboriginal and Torres Strait Islander communities to determine if, when, where and how they can use their resources, knowledge and skills to support the priorities of communities.
Adopting a genuine partnership approach requires not duplicating or competing with existing Aboriginal or Torres Strait Islander community-controlled family and child support services. SNAICC has developed a separate resource on approaches to partnership in the context of applications for grant funding that can be accessed at www.snaicc.org.au.
Before embarking on a new program or policy, use the abovementioned strategies to engage in a respectful and meaningful dialogue with Aboriginal and Torres Strait Islander organisations so that you understand the existing community strengths and needs. Doing this should inform you about whether a new program or policy is needed and, if so, what partnership support – if any – Aboriginal and Torres Strait Islander organisations will want and need to design and deliver it.
Taking the time to listen to and learn from Aboriginal and Torres Strait Islander peoples about what supports they need from partners is crucial for achieving self-determination. Genuine listening and learning should put non-Indigenous organisations in a position where they can answer the question: what financial and other resource support can we provide and share to support Aboriginal and Torres Strait Islander communities in their efforts to improve safety and wellbeing for children and families?
Examples of resources that could be shared in a partnership include:
- Knowledge and expertise
- Staff training
- Income
- Intellectual property
- Policies and accreditations
- Insurance
- Office space
- IT & financial systems
- Networks
- Recruiting project staff
- Fundraising
- Back office staff
SNAICC has created a capacity transfer tool to support organisations in planning for capacity transfer in partnership across the domains of people, culture, structure, systems and leadership. This tool is available on p25 of the SNAICC Partnership Training Manual.
IMPORTANT: Don’t assume that an Aboriginal and Torres Strait Islander organisation will necessarily need or want your support. Begin a dialogue and genuinely listen to determine whether you can provide assistance and what support is most needed.
|
GENUINELY LISTENING TO AND UNDERSTANDING THE NEEDS OF LOCAL ABORIGINAL AND TORRES STRAIT ISLANDER COMMUNITIES TAKES WORK Some of the challenges expressed in SNAICC’s 2019 partnership survey1 , by organisations currently in partnerships: |
‘Consistent communication due to both services being busy and not having the capacity to meet regularly is our biggest challenge.’ |
|---|---|
| ‘We could be more connected, but changes of staff and everyday busy-ness gets in the way of regularly connecting.’ | |
| ‘Unrealistic expectations, misunderstanding of roles and shifting of common purpose is a challenge.’ |
|
HELPFUL HINTS! Some of the things that have helped partnerships to flourish, expressed in SNAICC’s 2019 partnership survey, by organisations currently in partnerships: |
Joint training and development of staff across both organisations and programs has been so helpful in our partnership.’ |
|---|---|
| ‘Our partnership is successful because of a mutual commitment to supporting parents and carers, to producing quality resources, aligned values, strong communication that includes clear plans, timelines, regular check-ins and addressing hiccups early.’ | |
| ‘Mutual respect and recognition of the strengths and needs of Aboriginal people and each organisation has been helpful.’ |
|
WHAT ELSE CAN WE TRY? Useful strategies to build the cultural competence that underpins genuine partnerships include: |
Have the ‘hard’ conversations with Aboriginal and Torres Strait Islander partners about where non-Indigenous organisations can support community aspirations and also where they should step aside so that the community can lead. |
|---|---|
| Develop a capacity building plan for the partnership. Remember that capacity benefits should flow both ways and any plan should recognise the strengths that all partners bring. SNAICC has developed a capacity transfer plan that is available on p25 of the SNAICC Partnership Training Manual. | |
| Share staff training opportunities across organisations so that key knowledge, skills and relationships can be built concurrently. | |
| Discuss and agree early on what the end point or future state of the partnership should be. What will the partnership look like when capacity transfer goals are reached? |
Reflective Exercise
In reflecting on the opportunity for capacity building, consider:
- Have you read the leading capacity-building documents?
- Are you committed to genuinely listening to and acting on the recommendations of your local Aboriginal and Torres Strait Islander community?
- To what extent are your programs being codesigned and delivered with Aboriginal and Torres Strait Islander organisations?
- How can you make active efforts to resource and support capacity development of Aboriginal and Torres Strait Islander community-controlled agencies?
- Are there resources you have that could be better allocated to support partnership goals?
Where To from Here?
Leading capacity-building documents identified by SNAICC include:
- SNAICC’s Partnership Training Manual that aims to support and sustain genuine interagency partnerships in service delivery for Aboriginal and Torres Strait Islander children and families.
- SNAICC’s Collective Impact Toolkit, which provides guidance on how communities and organisations can work together to change outcomes for children and families, while respecting and supporting the role of Aboriginal and Torres Strait Islander peoples and organisations in leading on responses to child and family needs.
- SNAICC’s Opening Doors Through Partnerships report, which provides practical steps that Aboriginal and Torres Strait Islander organisations, non-Indigenous service providers and government can take to develop and support genuine partnerships that address Aboriginal and Torres Strait Islander needs. The report profiles case studies of good partnership development from across Australia, including interviews with service providers.
Strategy 4: Establish the Processes, Governance Structures and Accountability Required for Effective and Sustainable Partnerships
A strong and enduring partnership requires the development of a clear and effective governance structure for the partnership and the establishment of processes that support and sustain the ongoing development of the partnership.
Particular attention needs to be paid to how the Aboriginal and Torres Strait Islander community is represented in partnership governance. This will differ depending on the context of your community and partnership. Sometimes it will be appropriate for the community to be represented through the relevant community-controlled organisation, and sometimes it will be important for other community leaders and Elders to be included. The Aboriginal and Torres Strait Islander organisation in your partnership will be best placed to advise on how Aboriginal and Torres Strait Islander governance works where you are.
In establishing a partnership governance structure, pay careful attention to issues of control and power balance. In many cases, and often for reasons relating to histories and the continuing realities of discrimination, Aboriginal and Torres Strait Islander parties have been disadvantaged in partnership negotiations. They may have fewer resources and less initial service delivery capacity than governments and larger non-Indigenous organisations. As a result, they may have less bargaining power.
Also pay particular attention to how commitments to self-determination and community capacity building are reflected, and how the governance structure seeks to address historical and continuing discrimination and resulting power imbalance.
As partnerships develop and especially as they become more involved and complex, it will be important to formalise partnership processes and integrate them into the way your organisation works. Establishing clear partnership processes and agreements can help to ensure that partnerships are not reliant on the relationships between particular individuals and can survive changes in staff and leadership. Important partnership processes include:
- Agreements on the values, principles, goals, roles, responsibilities and activities of the partnership (see the tips for agreement making under Strategy 2 above)
- Regular meetings for partnership planning and review at all levels, from partnership governance, to individual activity planning between staff
- Integrating partnership processes into the policies and procedures of each organisation
- Formalising arrangements for resource and staff sharing
Taking a bottom-up, collaborative and participatory approach to the evaluation of your partnerships, and any programs that arise from them, is important for ensuring that you are collaborating and sharing power. Participatory models of evaluation enable Aboriginal and Torres Strait Islander communities to be involved in defining the criteria for what makes a successful program and partnership and to contribute to the assessment of progress and the making of plans to improve the partnership work.
|
ESTABLISHING AND MAINTAINING EFFECTIVE GOVERNANCE STRUCTURES AND PARTNERSHIP PROCESSES CAN SOMETIMES BE TRICKY Some of the challenges expressed in SNAICC’s 2019 partnership survey1 , by organisations currently in partnerships: |
‘Actually getting things happening has been a challenge. Day-to-day pressures impact on joint delivery. Recruitment issues pose additional challenges in remote areas.’ |
|---|---|
| ‘Our organisation is large and very resource rich, and is often leant on too much. It is a lesson for us all to stick to the parameters of a partnership – the roles and responsibilities being clear and agreed to by all parties is important.’ | |
| ‘Some regulations and compliance requirements are not culturally reflective and we have to consider other ways to support learnings and procedures to overcome this.’ |
|
HELPFUL HINTS! Some of the things that have helped partnerships to flourish, expressed in SNAICC’s 2019 partnership survey, by organisations currently in partnerships: |
‘Regular meetings, open communication and flexibility in regards to service delivery has worked.’ |
|---|---|
| ‘Transparent and clear goals and intentions which are documented by MOU and based on mutual respect is important.’ | |
| ‘Collaboration, shared learnings and capacity building, as well as formalising some processes is useful.’ |
|
WHAT ELSE CAN WE TRY? Useful strategies to build the cultural competence that underpins genuine partnerships include: |
Establish an MOU that sets out the values, principles, goals and activities that make up your partnership. Refer to the tips for agreement making under Strategy 2 above. |
|---|---|
| Consult with Aboriginal and Torres Strait Islander partners on how the community should be represented in the governance of the partnership and what roles community members can play in the partnership work. | |
| Develop a participatory partnership evaluation strategy that creates opportunities to discuss together what your goals are, how you will achieve them, how you will measure and reflect on progress, and how you will improve in response to what you learn. | |
| Allocate resources to partnership development and review processes. Consider whether independent facilitation might support development of partnerships and reflection on partnership work. |
Reflective Exercise
- Have you read the leading governance, process and accountability documents?
- What should the partnership governance structure look like for your partnership?
- How should the Aboriginal and Torres Strait Islander community be represented in the governance of the partnership?
- Does the balance need to shift over time with capacity development of the partners?
Where To from Here?
Leading partnership governance, process and accountability documents identified by SNAICC include:
- The Australian Institute for Family Studies report Evaluating the Outcomes of Programs for Indigenous Families and Communities has some useful guidance on participatory models of evaluation.
- AbSec and SNAICC’s Developing Capacity Through Partnerships resource which profiles the process of establishing capacity building partnerships for the development of Aboriginal community-controlled out-of-home care services in New South Wales.
- Noongar Child and Family Wellbeing Council and WACOSS Partnering with Aboriginal Community Controlled Organisations to deliver trusted services with stronger outcomes for Aboriginal people highlights values and practices for fair and equal partnerships and the means to measure their success, holding parties to account for their commitments.
- SNAICC’s Partnership Training Manual, that aims to support and sustain genuine interagency partnerships in service delivery for Aboriginal and Torres Strait Islander children and families.
- SNAICC’s Working and Walking Together resource includes a chapter, which provides guidance on undertaking action research with Aboriginal and Torres Strait Islander communities.
Additional Useful Resources
Want to know more about building and maintaining partnerships? The following resources are available online, and can help:
- SNAICC’s Opening Doors Through Partnerships report provides practical steps that Aboriginal and Torres Strait Islander organisations, non-Indigenous service providers and government can take to develop and support genuine partnerships that address Aboriginal and Torres Strait Islander needs. The report profiles case studies of good partnership development from across Australia, including interviews with service providers.
- SNAICC’s Working and Walking Together resource: supports family relationships services to work with Aboriginal and Torres Strait Islander Families and Organisations.
- SNAICC’s online Partnership Audit Tool provides guidance and exercises to assist you in establishing partnerships and reviewing their strength.
- SNAICC’s Partnership Training Manual is an interactive guide that aims to support and sustain genuine inter-agency partnerships in service delivery for Aboriginal and Torres Strait Islander children and families.
- SNAICC’s Whose Voice Counts? Aboriginal and Torres Strait Islander participation in child protection decision-making research report outlines the central importance and elements of Indigenous participation to quality and effective child protection decision-making for Indigenous children.
- APO NT Partnership Principles are designed to guide the development of a partnership-centred approach for non-Indigenous organisations engaging in the delivery of services or development initiatives in Aboriginal communities.
- ACOSS Principles for a Partnership-Centred Approach are designed to guide the development of a partnership-centred approach between Aboriginal and Torres Strait Islander and non-Indigenous NGOs in tendering for program funds and engaging in the delivery of services or development initiatives in Aboriginal and Torres Strait Islander communities.
- Noongar Child and Family Wellbeing Council and WACOSS Partnering with Aboriginal Community Controlled Organisations to deliver trusted services with stronger outcomes for Aboriginal people highlights values and practices for fair and equal partnerships and the means to measure their success, holding parties to account for their commitments.
- Victorian Aboriginal Child Care Agency’s (VACCA) Building Respectful Partnerships – The Commitment to Aboriginal Cultural Competence in Child and Family Services is a practice guide on building Aboriginal cultural competence.
Reference List
- Australian Institute of Family Studies, Parenting in the Early Years: Effectiveness of Parenting Support Programs for Indigenous Families (2012) < https://www. aihw.gov. au/getmedia/0e01fe6d-04b4-4ee9-bcba2614fdf27cc1/ctgc-rs16.pdf.aspx?inline=true>.
- Australian Institute of Health and Welfare, Children living in households with members of the Stolen Generations (2019) < https://www. aihw.gov.au/getmedia/a364d8f1-eeee-43c3- b91e-0fb31ebecf30/AIHW214-Children-andStolen-Generation.pdf.aspx?inline=true>.
- Australian National Audit Office (ANAO). (2012). Capacity Development for Indigenous Service Delivery, Audit Report No. 26, 2011-2012. Canberra: Commonwealth of Australia • Australian Early Development Census, Australian Early Development Census National Report 2019, Canberra: Commonwealth of Australia.
- Chandler, M., & Lalonde, C. (1998). Cultural Continuity as a Hedge Against Suicide in Canada’s First Nations, retrieved 20 August 2019 from: http://web.uvic.ca/~lalonde/ manuscripts/1998TransCultural.pdf.
- Commonwealth of Australia, Bringing them Home: Report of the National Inquiry into the Separation of Aboriginal and Torres Strait Islander Children from their Families (1997).
- SNAICC, The Family Matters Report 2019 (2019), Melbourne.
- Lavoie, J. et al (2010). Have investments in on-reserve health services and initiatives promoting community control improved First Nations’ health in Manitoba?, Social Science and Medicine, 71(4), August, 717.
- SNAICC, Opening Doors Through Partnerships (2012), Melbourne.
- The Victorian Aboriginal Child Care Agency, Aboriginal Cultural Competency Framework, Produced for the Victorian Government Department of Human Services (2008), p.24.
- United Nations, United Nations Convention on the Rights of the Child, (1989).
- United Nations, United Nations Declaration on the Rights of Indigenous Peoples (2011).
- Ware, V. (2012), Improving access to urban and regional early childhood services. Resource sheet No. 17. Produced for the Closing the Gap Clearinghouse. Canberra, ACT / Melbourne, Vic.: Australian Institute of Health and Welfare / Australian Institute of Family Studies.
- Wild, R., and Anderson, P. (2007). Little Children are Sacred, Report of the Northern Territory Board of Inquiry into the Protection of Aboriginal Children from Sexual Abuse, Darwin: Northern Territory Government
- Winangali and Ipsos Australia, Evaluation – Aboriginal and Torres Strait Islander Family-led Decision Making Trials (2017).

Rabinowitz, P. (n.d.). Section 6: Participatory evaluation. Community Tool Box.
Experienced community builders know that involving stakeholders - the people directly connected to and affected by their projects - in their work is tremendously important. It gives them the information they need to design, and to adjust or change, what they do to best meet the needs of the community and of the particular populations that an intervention or initiative is meant to benefit. This is particularly true in relation to evaluation.
As we have previously discussed, community-based participatory research can be employed in describing the community, assessing community issues and needs, finding and choosing best practices, and/or evaluation. We consider the topic of participatory evaluation important enough to give it a section of its own, and to show how it fits into the larger participatory research picture.
It's a good idea to build stakeholder participation into a project from the beginning. One of the best ways to choose the proper direction for your work is to involve stakeholders in identifying real community needs, and the ways in which a project will have the greatest impact. One of the best ways to find out what kinds of effects your work is having on the people it's aimed at is to include those on the receiving end of information or services or advocacy on your evaluation team
Often, you can see most clearly what's actually happening through the eyes of those directly involved in it - participants, staff, and others who are involved in taking part in and carrying out a program, initiative, or other project. Previously, we have discussed how you can involve those people in conducting research on the community and choosing issues to address and directions to go in. This section is about how you can involve them in the whole scope of the project, including its evaluation, and how that's likely to benefit the project's final outcomes.
What is Participatory Evaluation?
When most people think of evaluation, they think of something that happens at the end of a project - that looks at the project after it's over and decides whether it was any good or not. Evaluation actually needs to be an integral part of any project from the beginning. Participatory evaluation involves all the stakeholders in a project - those directly affected by it or by carrying it out - in contributing to the understanding of it, and in applying that understanding to the improvement of the work.
Participatory evaluation, as we shall see, isn't simply a matter of asking stakeholders to take part. Involving everyone affected changes the whole nature of a project from something done for a group of people or a community to a partnership between the beneficiaries and the project implementers. Rather than powerless people who are acted on, beneficiaries become the co-pilots of a project, making sure that their real needs and those of the community are recognized and addressed. Professional evaluators, project staff, project beneficiaries or participants, and other community members all become colleagues in an effort to improve the community's quality of life.
This approach to planning and evaluation isn't possible without mutual trust and respect. These have to develop over time, but that development is made more probable by starting out with an understanding of the local culture and customs - whether you're working in a developing country or in an American urban neighborhood. Respecting individuals and the knowledge and skills they have will go a long way toward promoting long-term trust and involvement.
The other necessary aspect of any participatory process is appropriate training for everyone involved. Some stakeholders may not even be aware that project research takes place; others may have no idea how to work alongside people from different backgrounds; and still others may not know what to do with evaluation results once they have them. We'll discuss all of these issues - stakeholder involvement, establishing trust, and training - as the section progresses.
The real purpose of an evaluation is not just to find out what happened, but to use the information to make the project better.
In order to accomplish this, evaluation should include examining at least two areas:
- Process. The process of a project includes the planning and logistical activities needed to set up and run it. Did we do a proper assessment beforehand so we would know what the real needs were? Did we use the results of the assessment to identify and respond to those needs in the design of the project? Did we set up and run the project within the timelines and other structures that we intended? Did we involve the people we intended to? Did we have or get the resources we expected? Were staff and others trained and prepared to do the work? Did we have the community support we expected? Did we record what we did accurately and on time? Did we monitor and evaluate as we intended?
- Implementation. Project implementation is the actual work of running it. Did we do what we intended? Did we serve or affect the number of people we proposed to? Did we use the methods we set out to use? Was the level of our activity what we intended (e.g., did we provide the number of hours of service we intended to)? Did we reach the population(s) we aimed at? What exactly did we provide or do? Did we make intentional or unintentional changes, and why?
- Outcomes. The project's outcomes are its results - what actually happened as a consequence of the project's existence. Did our work have the effects we hoped for? Did it have other, unforeseen effects? Were they positive or negative (or neither)? Do we know why we got the results we did? What can we change, and how, to make our work more effective?
Many who write about participatory evaluation combine the first two of these areas into process evaluation, and add a third - impact evaluation - in addition to outcome evaluation. Impact evaluation looks at the long-term results of a project, whether the project continues, or does its work and ends.
Rural development projects in the developing world, for example, often exist simply to pass on specific skills to local people, who are expected to then both practice those skills and teach them to others. Once people have learned the skills - perhaps particular cultivation techniques, or water purification - the project ends. If in five or ten years, an impact evaluation shows that the skills the project taught are not only still being practiced, but have spread, then the project's impact was both long-term and positive.
In order for these areas to be covered properly, evaluation has to start at the very beginning of the project, with assessment and planning.
In a participatory evaluation, stakeholders should be involved in:
- Naming and framing the problem or goal to be addressed
- Developing a theory of practice (process, logic model) for how to achieve success
- Identifying the questions to ask about the project and the best ways to ask them - these questions will identify what the project means to do, and therefore what should be evaluated
What's the real goal, for instance, of a program to introduce healthier foods in school lunches? It could be simply to convince children to eat more fruits, vegetables, and whole grains. It could be to get them to eat less junk food. It could be to encourage weight loss in kids who are overweight or obese. It could simply be to educate them about healthy eating, and to persuade them to be more adventurous eaters. The evaluation questions you ask both reflect and determine your goals for the program. If you don't measure weight loss, for instance, then clearly that's not what you're aiming at. If you only look at an increase in children's consumption of healthy foods, you're ignoring the fact that if they don't cut down on something else (junk food, for instance), they'll simply gain weight. Is that still better than not eating the healthy foods? You answer that question by what you choose to examine - if it is better, you may not care what else the children are eating; if it's not, then you will care.
- Collecting information about the project
- Making sense of that information
- Deciding what to celebrate, and what to adjust or change, based on information from the evaluation
Why Would (and Why Wouldn’t) You Use Participatory Evaluation?
Why would you use participatory evaluation? The short answer is that it's often the most effective way to find out what you need to know, both at the beginning of and throughout the course of a project. In addition, it carries benefits for both individual participants and the community that other methods don't.
Some of the major advantages of participatory evaluation:
- It gives you a better perspective on both the initial needs of the project's beneficiaries, and on its ultimate effects. If stakeholders, including project beneficiaries, are involved from the beginning in determining what needs to be evaluated and why - not to mention what the focus of the project needs to be - you're much more likely to aim your work in the right direction, to correctly determine whether your project is effective or not, and to understand how to change it to make it more so.
- It can get you information you wouldn't get otherwise. When project direction and evaluation depend, at least in part, on information from people in the community, that information will often be more forthcoming if it's asked for by someone familiar. Community people interviewing their friends and neighbors may get information that an outside person wouldn't be offered.
- It tells you what worked and what didn't from the perspective of those most directly involved - beneficiaries and staff. Those implementing the project and those who are directly affected by it are most capable of sorting out the effective from the ineffective.
- It can tell you why something does or doesn't work. Beneficiaries are often able to explain exactly why they didn't respond to a particular technique or approach, thus giving you a better chance to adjust it properly.
- It results in a more effective project. For the reasons just described, you're much more apt to start out in the right direction, and to know when you need to change direction if you haven't. The consequence is a project that addresses the appropriate issues in the appropriate way, and accomplishes what it sets out to do.
- It empowers stakeholders. Participatory evaluation gives those who are often not consulted - line staff and beneficiaries particularly - the chance to be full partners in determining the direction and effectiveness of a project.
- It can provide a voice for those who are often not heard. Project beneficiaries are often low-income people with relatively low levels of education, who seldom have - and often don't think they have a right to - the chance to speak for themselves. By involving them from the beginning in project evaluation, you assure that their voices are heard, and they learn that they have the ability and the right to speak for themselves.
- It teaches skills that can be used in employment and other areas of life. In addition to the development of basic skills and specific research capabilities, participatory evaluation encourages critical thinking, collaboration, problem-solving, independent action, meeting deadlines...all skills valued by employers, and useful in family life, education, civic participation, and other areas.
- It bolsters self-confidence and self-esteem in those who may have little of either. This category can include not only project beneficiaries, but also others who may, because of circumstance, have been given little reason to believe in their own competence or value to society. The opportunity to engage in a meaningful and challenging activity, and to be treated as a colleague by professionals, can make a huge difference for folks who are seldom granted respect or given a chance to prove themselves.
- It demonstrates to people ways in which they can take more control of their lives. Working with professionals and others to complete a complex task with real-world consequences can show people how they can take action to influence people and events.
- It encourages stakeholder ownership of the project. If those involved feel the project is theirs, rather than something imposed on them by others, they'll work hard both in implementing it, and in conducting a thorough and informative evaluation in order to improve it.
- It can spark creativity in everyone involved. For those who've never been involved in anything similar, a participatory evaluation can be a revelation, opening doors to a whole new way of thinking and looking at the world. To those who have taken part in evaluation before, the opportunity to exchange ideas with people who may have new ways of looking at the familiar can lead to a fresh perspective on what may have seemed to be a settled issue.
- It encourages working collaboratively. For participatory evaluation to work well, it has to be viewed by everyone involved as a collaboration, where each participant brings specific tools and skills to the effort, and everyone is valued for what she can contribute. Collaboration of this sort not only leads to many of the advantages described above, but also fosters a more collaborative spirit for the future as well, leading to other successful community projects.
- It fits into a larger participatory effort. When community assessment and the planning of a project have been a collaboration among project beneficiaries, staff, and community members, it only makes sense to include evaluation in the overall plan, and to approach it in the same way as the rest of the project. In order to conduct a good evaluation, its planning should be part of the overall planning of the project. Furthermore, participatory process generally matches well with the philosophy of community-based or grass roots groups or organizations.
With all these positive aspects, participatory evaluation carries some negative ones as well. Whether its disadvantages outweigh its advantages depend on your circumstances, but whether you decide to engage in it or not, it's important to understand what kinds of drawbacks it might have.
The significant disadvantages of participatory evaluation include:
- It takes more time than conventional process. Because there are so many people with different perspectives involved, a number of whom have never taken part in planning or evaluation before, everything takes longer than if a professional evaluator or a team familiar with evaluation simply set up and conducted everything. Decision-making involves a great deal of discussion, gathering people together may be difficult, evaluators need to be trained, etc.
- It takes the establishment of trust among all participants in the process. If you're starting something new (or, all too often, even if the project is ongoing), there are likely to be issues of class distinction, cultural differences, etc., dividing groups of stakeholders. These can lead to snags and slowdowns until they're resolved, which won't happen overnight. It will take time and a good deal of conscious effort before all stakeholders feel comfortable and confident that their needs and culture are being addressed.
- You have to make sure that everyone's involved, not just "leaders" of various groups. All too often, "participatory" means the participation of an already-existing power structure. Most leaders are actually that - people who are most concerned with the best interests of the group, and whom others trust to represent them and steer them in the direction that best reflects those interests. Sometimes, however, leaders are those who push their way to the front, and try to confirm their own importance by telling others what to do.
- By involving only leaders of a population or community, you run the risk of losing - or never gaining - the confidence and perspective of the rest of the population, which may dislike and distrust a leader of the second type, or may simply see themselves shut out of the process.. They may see the participatory evaluation as a function of authority, and be uninterested in taking part in it. Working to recruit "regular" people as well as, or instead of, leaders may be an important step for the credibility of the process. But it's a lot of work and may be tough to sell.
- You have to train people to understand evaluation and how the participatory process works, as well as teaching them basic research skills. There are really a number of potential disadvantages here. The obvious one is that of time, which we've already raised - training takes time to prepare, time to implement, and time to sink in. Another is the question of what kind of training participants will respond to. Still another concerns recruitment - will people be willing to put in the time necessary to prepare them for the process, let alone the time for the process itself?
- You have to get buy-in and commitment from participants. Given what evaluators will have to do, they need to be committed to the process, and to feel ownership of it. You have to structure both the training and the process itself to bring about this commitment.
- People's lives - illness, child care and relationship problems, getting the crops in, etc. - may cause delays or get in the way of the evaluation. Poor people everywhere live on the edge, which means they're engaged in a delicate balancing act. The least tilt to one side or the other - a sick child, too many days of rain in a row - can cause a disruption that may result in an inability to participate on a given day, or at all. If you're dealing with a rural village that's dependent on agriculture, for instance, an accident of weather can derail the whole process, either temporarily or permanently.
- You may have to be creative about how you get, record, and report information. If some of the participants in an evaluation are non- or semi-literate, or if participants speak a number of different languages (English, Spanish, and Lao, for instance), a way to record information will have to be found that everyone can understand, and that can, in turn, be understood by others outside the group.
- Funders and policy makers may not understand or believe in participatory evaluation. At worst, this can lose you your funding, or the opportunity to apply for funding. At best, you'll have to spend a good deal of time and effort convincing funders and policy makers that participatory evaluation is a good idea, and obtaining their support for your effort.
Some of these disadvantages could also be seen as advantages: the training people receive blends in with their development of new skills that can be transferred to other areas of life, for instance; coming up with creative ways to express ideas benefits everyone; once funders and policy makers are persuaded of the benefits of participatory process and participatory evaluation, they may encourage others to employ it as well. Nonetheless, all of these potential negatives eat up time, which can be crucial. If it's absolutely necessary that things happen quickly (which is true not nearly as often as most of us think it is), participatory evaluation is probably not the way to go.
When Might You Use Participatory Evaluation?
So when do you use participatory evaluation? Some of the reasons you might decide it’s the best choice for your purposes:
- When you're already committed to a participatory process for your project. Evaluation planning can be included and collaboratively designed as part of the overall project plan.
- When you have the time, or when results are more important than time. As should be obvious from the last part of this section, one of the biggest drawbacks to participatory evaluation is the time it takes. If time isn't what's most important, you can gain the advantages of a participatory evaluation without having to compensate for many of the disadvantages.
- When you can convince funders that it's a good idea. Funders may specify that they want an outside evaluation, or they may simply be dubious about the value of participatory evaluation. In either case, you may have some persuading to do in order to be able to use a participatory process. If you can get their support, however, funders may like the fact that participatory evaluation is often less expensive, and that it has added value in the form of empowerment and transferable skills.
- When there may be issues in the community or population that outside evaluators (or program providers, for that matter) aren't likely to be aware of. Political, social, and interpersonal factors in the community can skew the results of an evaluation, and without an understanding of those factors and their history, evaluators may have no idea that what they're finding out is colored in any way. Evaluators who are part of the community can help sort out the influence of these factors, and thus end up with a more accurate evaluation.
- When you need information that it will be difficult for anyone outside the community or population to get. When you know that members of the community or population in question are unwilling to speak freely to anyone from outside, participatory evaluation is a way to raise the chances that you'll get the information you need.
- When part of the goal of the project is to empower participants and help them develop transferable skills. Here, the participatory evaluation, as it should in any case, becomes a part of the project itself and its goals.
- When you want to bring the community or population together. In addition to fostering a collaborative spirit, as we've mentioned, a participatory evaluation can create opportunities for people who normally have little contact to work together and get to know one another. This familiarity can then carry over into other aspects of community life, and even change the social character of the community over the long term.
Who Should Be Involved in Participatory Evaluation?
We've referred continually to stakeholders - the people who are directly affected by the project being evaluated. Who are the stakeholders? That varies from project to project, depending on the focus, the funding, the intended outcomes, etc.
There are a number of groups that are generally involved, including:
- Participants or beneficiaries. The people whom the project is meant to benefit. That may be a specific group (people with a certain medical condition, for instance), a particular population (recent Southeast Asian immigrants, residents of a particular area), or a whole community. They may be actively receiving a service (e.g., employment training) or may simply stand to benefit from what the project is doing (violence prevention in a given neighborhood). These are usually the folks with the greatest stake in the project's success, and often the ones with the least experience of evaluation.
- Project line staff and/or volunteers. The people who actually do the work of carrying out the project. They may be professionals, people with specific skills, or community volunteers. They may work directly with project beneficiaries as mentors, teachers, or health care providers; or they may advocate for immigrant rights, identify open space to be preserved, or answer the phone and stuff envelopes. Whoever they are, they often know more about what they're doing than anyone else, and their lives can be affected by the project as much as those of participants or beneficiaries.
- Administrators. The people who coordinate the project or specific aspects of it. Like line staff and volunteers, they know a lot about what's going on, and they're intimately involved with the project every day.
- Outside evaluators, if they're involved. In many cases, outside evaluators are hired to run participatory evaluations. The need for their involvement is obvious.
- Community officials. You may need the support of community leaders, or you may simply want to give them and other participants the opportunity to get to know one another in a context that might lead to better understanding of community needs.
- Others whose lives are affected by the project. The definition of this group varies greatly from project to project. In general, it refers to people whose jobs or other aspects of their lives will be changed either by the functioning of the project itself, or by its outcomes.
An example would be landowners whose potential use of their land would be affected by an environmental initiative or a neighborhood plan.
How Do You Conduct a Participatory Evaluation?
Participatory evaluation encompasses elements of designing the project as well as evaluating it. What you evaluate depends on what you want to know and what you're trying to do. Identifying the actual evaluation questions sets the course of the project just as surely as a standardized testing program guides teaching. When these questions come out of an assessment in which stakeholders are involved, the evaluation is one phase of a community-based participatory research process.
A participatory evaluation really has two stages: One comprises finding and training stakeholders to act as participant evaluators. The second - some of which may take place before or during the first stage - encompasses the planning and implementation of the project and its evaluation, and includes six steps:
- Naming and framing the issue
- Developing a theory of practice to address it
- Deciding what questions to ask, and how to ask them to get the information you need
- Collecting information
- Analyzing the information you've collected
- Using the information to celebrate what worked, and to adjust and improve the project
We'll examine both of these stages in detail.
Finding and Training Stakeholders to Act as Participant Evaluators
Unfortunately, this stage isn't simply a matter of announcing a participatory evaluation and then sitting back while people beat down the doors to be part of it. In fact, it may be one of the more difficult aspects of conducting a participatory evaluation.
Here's where the trust building we discussed earlier comes into play. The population you're working with may be distrustful of outsiders, or may be used to promises of involvement that turn out to be hollow or simply ignored. They may be used to being ignored in general, and/or offered services and programs that don't speak to their real needs. If you haven't already built a relationship to the point where people are willing to believe that you'll follow through on what you say, now is the time to do it. It may take some time and effort - you may have to prove that you'll still be there in six months - but it's worth it. You're much more likely to have a successful project, let alone a successful evaluation, if you have a relationship of mutual trust and respect.
But let's assume you have that step out of the way, and that you've established good relationships in the community and among the population you're working with, as well as with staff of the project. Let's assume as well that these folks know very little, if anything, about participatory evaluation. That means they'll need training in order to be effective.
If, in fact, your evaluation is part of a larger participatory effort, the question arises as to whether to simply employ the same team that did assessments and/or planned the project, perhaps with some additions, as evaluators. That course of action has both pluses and minuses. The team is already assembled, has developed a method of working together, has some training in research methods, etc., so that they can hit the ground running - obviously a plus.
The fact that they have a big stake in seeing the project be successful can work either way: they may interpret their findings in the best possible light, or even ignore negative information; or they may be eager to see exactly where and how to adjust the work to make it go better.
Another issue is burnout. Evaluation will mean more time in addition to what an assessment and planning team has already put in. While some may be more than willing to continue, many may be ready for a break (or may be moving on to another phase of their lives). If the possibility of assembling a new team exists, it will give those who've had enough the chance to gracefully withdraw.
How you handle this question will depend on the attitudes of those involved, how many people you actually have to draw on (if the recruitment of the initial team was really difficult, you may not have a lot of choices), and what people committed to.
Recruit Participant Evaluators
There are many ways to accomplish this. In some situations, it makes the most sense to put out a general call for volunteers; in others, to approach specific individuals who are likely - because of their commitment to the project or to the population - to be willing. Alternatively, you might approach community leaders or stakeholders to suggest possible evaluators.
Some basic guidelines for recruitment include:
- Use communication channels and styles that reach the people you're aiming at
- Make your message as clear as possible
- Use plain English and/or whatever other language(s) the population uses
- Put your message where the audience is
- Approach potential participants individually where possible - if you can find people they know to recruit them, all the better
- Explain what people may gain from participation
- Be clear that they're being asked because they already have the qualities that are necessary for participation
- Encourage people, but also be honest about the amount and extent of what needs to be done
- Work out with participants what they're willing and able to do
- Try to arrange support - child care, for example - to make participation easier 100
- Ask people you've recruited to recommend - or recruit – others
In general, it's important for potential participant evaluators - particularly those whose connection to the project isn't related to their employment - to understand the commitment involved. An evaluation is likely to last a year, unless the project is considerably shorter than that, and while you might expect and plan for some dropouts, most of the team needs to be available for that long.
In order to make that commitment easier, discuss with participants what kinds of support they'll need in order to fulfill their commitment - child care and transportation, for instance - and try to find ways to provide it. Arrange meetings at times and places that are easiest for them (and keep the number of meetings to a minimum). For participants who are paid project staff, the evaluation should be considered part of their regular work, so that it isn't an extra, unpaid, burden that they feel they can't refuse.
Be careful to try to put together a team that's a cross-section of the stakeholder population. As we've already discussed, if you recruit only "leaders" from among the beneficiary population, for instance, you may create resentment in the rest of the group, not get a true perspective of the thinking or perceptions of that group, and defeat the purpose of the participatory nature of the evaluation as well. Even if the leaders are good representatives of the group, you may want to broaden your recruitment in the hopes of developing more community leadership, and empowering those who may not always be willing to speak out.
Train Participant Evaluators
Participants, depending on their backgrounds, may need training in a number of areas. They may have very little experience in attending and taking part in meetings, for instance, and may need to start there. They may benefit from an introduction to the idea of participatory evaluation, and how it works. And they'll almost certainly need some training in data gathering and analysis.
How training gets carried out will vary with the needs and schedules of participants and the project. It may take place in small chunks over a relatively long period of time - weeks or months - might happen all at once in the course of a weekend retreat, or might be some combination. There's no right or wrong way here. The first option will probably make it possible for more people to take part; the second allows for people to get to know one another and bond as a team, and a combination might allow for both.
By the same token, there are many training methods, any or all of which might be useful with a particular group. Training in meeting skills - knowing when and how to contribute and respond, following discussion, etc. - may best be accomplished through mentoring, rather than instruction. Interviewing skills may best be learned through roleplaying and other experiential techniques. Some training - how to approach local people, for example - might best come from participants themselves.
Some of the areas in which training might be necessary:
The participatory evaluation process. How participatory evaluation works, its goals, the roles people may play in the process, what to expect.
- Meeting skills. Following discussion, listening skills, handling disagreement or conflict, contributing and responding appropriately, general ground rules and etiquette, etc.
- Interviewing. Putting people at ease, body language and tone of voice, asking open-ended and follow-up questions, recording what people say and other important information, handling interruptions and distractions, group interviews.
- Observation. Direct vs. participant observation, choosing appropriate times and places to observe, relevant information to include, recording observations.
- Recording information and reporting it to the group. What interviewees and those observed say and do, the non-verbal messages they send, who they are (age, situation, etc.), what the conditions were, the date and time, any other factors that influenced the interview or observation.
- Analyzing information. Critical thinking, what kinds of things statistics tell you, other things to think about.
For people for whom writing isn't comfortable, where writing isn't feasible, or where language is a barrier, there should be alternative recording and reporting methods. Drawings, maps, diagrams, tape recording, videos, or other imaginative ways of remembering exactly what was said or observed can be substituted, depending on the situation. In interviews, if audio or video recording is going to be used, it's important to get the interviewee's permission first - before the interviewer shows up with the equipment, so that there are no misunderstandings.
Planning and Implementing the Project and its Evaluation

There's an assumption here that all phases of a project will be participatory, so that not only its evaluation, but its planning and the assessment that leads to it also involve stakeholders (not necessarily the same ones who act as evaluators). If stakeholders haven't been involved from the beginning, they don't have the deep understanding of the purposes and structure of a project that they'd have of one they've helped form. The evaluation that results, therefore, is likely to be less perceptive - and therefore less valuable - than one of a project they've been involved in from the start.
Naming and Framing the Problem or Goal to be Addressed
Identifying what you're evaluating defines what the project is meant to address and accomplish. Community representatives and stakeholders, all those with something to gain or lose, work together to develop a shared vision and mission. By collecting information about community concerns and identifying available assets, communities can understand which issues to focus a project on.
Naming a problem or goal refers to identifying the issue that needs to be addressed. Framing it has to do with the way we look at it. If youth violence is conceived of as strictly a law enforcement problem, for instance, that framing implies specific ways of solving it: stricter laws, stricter enforcement, zero tolerance for violence, etc. If it's framed as a combination of a number of issues - availability of hand guns, unemployment and drug use among youth, social issues that lead to the formation of gangs, alienation and hopelessness in particular populations, poverty, etc. - then solutions may include employment and recreation programs, mentoring, substance abuse treatment, etc., as well as law enforcement. The more we know about a problem, and the more different perspectives we can include in our thinking about it, the more accurately we can frame it, and the more likely we are to come up with an effective solution.
Developing a Theory of Practice to Address the Problem
How do you conduct a community effort so that it has a good chance of solving the problem at hand? Many communities and organizations answer this question by throwing uncoordinated programs at the problem, or by assuming a certain approach (law enforcement, as in our example, for instance) will take care of it. In fact, you have to have a plan for creating, implementing, evaluating, adjusting, and maintaining a solution if you want it to work.
Whatever you call this plan - a theory of practice, a logic model, or simply an approach or process - it should be logical, consistent, consider all the areas that need to be coordinated in order for it to work, and give you an overall guideline and a list of steps to follow in order to carry it out.
Once you’ve identified an issue, for instance, one possible theory of practice might be:
- Form a coalition of organizations, agencies, and community members concerned with the problem.
- Recruit and train a participatory research team which includes representatives of all stakeholder groups.
- The team collects both statistical and qualitative, first-hand information about the problem, and identifies community assets that might help in addressing it.
- Use the information you have to design a solution that takes into account the problem's complexity and context. This might be a single program or initiative, or a coordinated, community-wide effort involving several organizations, the media, and individuals. If it's closer to the latter, that's part of the complexity you have to take into account. Coordination has to be part of your solution, as do ways to get around the bureaucratic roadblocks that might occur and methods to find the financial and personnel resources you need.
- Implement the solution.
- Carry out monitoring and evaluation that will give you ongoing feedback about how well you're meeting objectives, and what you should change to improve your solution.
- Use the information from the evaluation to adjust and improve the solution.
- Go back to # 2 and do as much of it again as you need to until the problem is solved, or - more likely, since many community problems never actually disappear - indefinitely in order to maintain and increase your gains.
Deciding What Evaluation Questions to Ask, And How to Ask Them to Get the Information You Need
As we've discussed, choosing the evaluation questions essentially guides the work. What you're really choosing here is what you're going to pay attention to. There could be significant results from your project that you're never aware of, because you didn't look for them - you didn't ask the questions to which those results would have been the answers. That's why it's so important to select questions carefully: they'll determine what you find.
Framing the problem is one element here - putting it in context, looking at it from all sides, stepping back from your own assumptions and biases to get a clearer and broader view of it. Another is envisioning the outcomes you want, and thinking about what needs to change, and how, in order to reach them.
Framing is important in this activity as well. If you want simply to reduce youth violence, stricter laws and enforcement might seem like a reasonable solution, assuming you're willing to stick with them forever; if you want not only to reduce or eliminate youth violence, but to change the climate that fosters it (i.e., long term social change), the solution becomes much broader and requires, as we pointed out above, much more than law enforcement. And a broader solution means more, and more complex, evaluation questions.
In the first case, evaluation questions might be limited to some variation of: "Were there more arrests and convictions of youthful offenders for violent crimes in the time period studied, as compared to the last period for which there were records before the new solution was put in place?" "Did youthful offenders receive harsher sentences than before?" "Was there a reduction in violent incidents involving youth?"
Looking at the broader picture, in addition to some of those questions, there might be questions about counseling programs for youthful offenders to change their attitudes and to help ease their transition back to civil society, drug and alcohol treatment, control of handgun sales, changing community attitudes, etc.
Collecting Information
This is the largest part, at least in time and effort, of implementing an evaluation.
Various evaluators, depending on the information needed, may conduct any or all of the following:
- Research into census or other public records, as well as news archives, library collections, the Internet, etc.
- Individual and/or group interviews
- Focus groups
- Community information-sharing sessions
- Surveys
- Direct or participant observation
In some cases - particularly with unschooled populations in developing countries - evaluators may have to find creative ways to draw out information. In some cultures, maps, drawings, representations ("If this rock is the headman's house..."), or even storytelling may be more revealing than the answers to straightforward questions.
Analyzing the Information You’ve Collected
Once you've collected all the information you need, the next step is to make sense of it. What do the numbers mean? What do people's stories and opinions tell you about the project? Did you carry out the process you'd planned? If not, did it make a difference, positive or negative?
In some cases, these questions are relatively easy to answer. If there were particular objectives for serving people, or for beneficiaries' accomplishments, you can quickly find out whether they were met or not. (We set out to serve 75 people, and we actually served 82. We anticipated that 50 would complete the program, and 61 actually completed.)
In other cases, it's much harder to tell what your information means. What if approximately half of interviewees say the project was helpful to them, and the other half say the opposite? A result like that may leave you doing some detective work. (Is there any ethnic, racial, geographic, or cultural pattern as to who is positive and who is negative? Whom did each group work with? Where did they experience the project, and how? Did members of each group have specific things in common?)
While collecting the information requires the most work and time, analyzing it is perhaps the most important step in conducting an evaluation. Your analysis tells you what you need to know in order to improve your project, and also gives you the evidence you need to make a case for continued funding and community support. It's important that it be done well, and that it make sense of odd results like that directly above. Here's where good training and good guidance in using critical thinking and other techniques come in.
In general, information-gathering and analysis should cover the three areas we discussed early in the section: process, implementation, and outcomes. The purpose here is both to provide information for improving the project and to provide accountability to funders and the community.
- Process. This concerns the logistics of the project. Was there good coordination and communication? Was the planning process participatory? Was the original timeline for each stage of the project - outreach, assessment, planning, implementation, evaluation - realistic? Were you able to find or hire the right people? Did you find adequate funding and other resources? Was the space appropriate? Did members of the planning and evaluation teams work well together? Did the people responsible do what they were expected to do? Did unexpected leaders emerge (in the planning group, for instance)?
- Implementation. Did you do what you set out to do - reach the number of people you expected to, use the methods you intended, provide the amount and kind of service or activity that you planned for? This part of the evaluation is not meant to assess effectiveness, but only whether the project was carried out as planned - i.e., what you actually did, rather than what you accomplished as a result. That comes next.
- Outcomes. What were the results of what you did? Did what you hoped for take place? If it did, how do you know it was a result of what you did, as opposed to some other factor(s)? Were there unexpected results? Were they negative or positive? Why did this all happen?
Using the Information to Celebrate What Worked, and to Adjust and Improve the Project
While accountability is important - if the project has no effect at all, for example, it's just wasted effort - the real thrust of a good evaluation is formative. That means it's meant to provide information that can help to continue to form the project, reshape it to make it better. As a result, the overall questions when looking at process, implementation, and outcomes are: What worked well? What didn't? What changes would improve the project?
Answering these questions requires further analysis, but should allow you to improve the project considerably. In addition to dropping or changing and adjusting those elements of the project that didn't work well, don't neglect those that were successful. Nothing's perfect; even effective approaches can be made better.
Don't forget to celebrate your successes. Celebration recognizes the hard work of everyone involved, and the value of your effort. It creates community support, and strengthens the commitment of those involved. Perhaps most important, it makes clear that people working together can improve the quality of life in the community.
There's a final element to participatory research and evaluation that can't be ignored. Once you've started a project and made it successful, you have to maintain it. The participatory research and evaluation has to continue - perhaps not with the same team(s), but with teams representative of all stakeholders. Conditions change, and projects have to adapt. Research into those conditions and continued evaluation of your work will keep that work fresh and effective.
If your project is successful, you may think your work is done. Think again - community problems are only solved as long as the solutions are actively practiced. The moment you turn your back, the conditions you worked so hard to change can start to return to what existed before The work - supported by participatory research and evaluation - has to go on indefinitely to maintain and increase the gains you've made.
In Summary
Participatory evaluation is a part of participatory research. It involves stakeholders in a community project in setting evaluation criteria for it, collecting and analyzing data, and using the information gained to adjust and improve the project.
Participatory process brings in the all-important multiple perspectives of those most directly affected by the project, who are also most likely to be tied into community history and culture. The information and insights they contribute can be crucial in a project's effectiveness. In addition, their involvement encourages community buy-in, and can result in important gains in skills, knowledge, and self-confidence and self-esteem for the researchers. All in all, participatory evaluation creates a win-win situation.
Conducting a participatory evaluation involves several steps:
- Recruiting and training a stakeholder evaluation team
- Naming and framing the problem
- Developing a theory of practice to guide the process of the work
- Asking the right evaluation questions
- Collecting information
- Analyzing information
- Using the information to celebrate and adjust your work
The final step, as with so many of the community-building strategies and actions described in the Community Tool Box, is to keep at it. Participatory research in general, and participatory evaluation in particular, has to continue as long as the work continues, in order to keep track of community needs and conditions, and to keep adjusting the project to make it more responsive and effective. And the work often has to continue indefinitely in order to maintain progress and avoid sliding back into the conditions or attitudes that made the project necessary in the first place.
