In this section you will learn to:
- Understand the drug classification system common used in Australia
- Identify the different types of drugs and their pharmacological properties, including signs and symptoms after administering them
- Identify and understand the effects of drugs on the user and their community
- Understand poly drug use, and how drug interactions affect the users
Supplementary materials relevant to this section:
- Reading B: Effects of Drugs on Brain Structure and Function: The Exposure Model

The previous section of this module provided you with an introduction of alcohol and other drugs use pattern, and the harms and impacts of AOD. You also learned about the different theoretical models used to explain substance use and its dependency. However, you will also need the pharmacological knowledge of drugs in order to obtain a clearer picture of your client’s AOD use and how AOD affects them both physically and psychologically. In this section, you will be introduced to the neurophysiology of addiction, the drug classification systems, and how drugs affect individuals who use them. You will also learn about the signs and symptoms of substance dependence as well as how the interaction between drugs can affect the individual (poly drug interaction).

Before moving on to the introduction of classifications of drugs, we will first learn about the neurophysiology of addiction. The different parts of our brain communicate via a network of neurons within the brain and throughout the nervous system. The nerve networks co-ordinate and regulate what we feel, think, and do.
Messages are typically transmitted between neurons by chemicals called neurotransmitters. These attach to a specialised site on the receiving neuron called a receptor in a manner similar to a ‘lock and key’ system. A specialised mechanism on the transmitting neuron called a ‘transporter’ has the ability to moderate or shut off the signal by recalling or recycling the neurotransmitters (NIDA, 2020).
A basic concept of this process is the ‘reward pathway’ which comprises the areas of the brain most involved in addiction. This reward pathway is designed to reward natural behaviours that are functional to human life (for example, exercising, eating, and social interaction). However, most drugs flood this pathway with dopamine, a neurotransmitter regulating movement, emotion, motivation, and feelings of pleasure. This results in pleasurable sensations and euphoria, which reinforce the drug’s continued use. Previously, researchers proposed that this surge in dopamine directly caused euphoria. However, recent research indicated that it is possible that dopamine reinforces individuals to perform pleasurable activities rather than causing the pleasure directly. (NIDA, 2020).
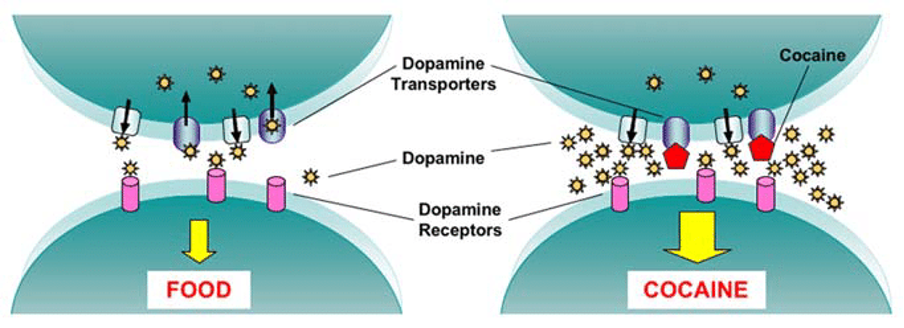
For example, the diagram below depicts the difference in dopamine uptake between natural processes such as eating and AOD use such as taking cocaine. The latter interferes with the normal action of dopamine by blocking its removal (or reuptake). The result is an excess of dopamine at the neurons and an overstimulation of receiving neurons experienced as pleasurable euphoria. The diagram below demonstrates this process:
Chronic use of psychoactive substances can eventually lead to significant changes in neurons and brain circuits. This leads to loss of self-control and ability to make sound decisions, while producing intense impulses (or cravings) to continue using AOD. Essentially, chronic substance use may lead to physical damage in the brain, resulting in a reduced ability to unlearn destructive behaviours related to substance use (NIDA, 2020).

Drug Cues
Due to continued drug use, cues in the individual’s daily routine or environment that are associated with drug use can trigger uncontrollable drug cravings. This “learned reflex” is due to the changes to the reward circuit in the individual’s brain. Interestingly, this reflex lasts for a very long time, even in individuals who have not administer any drugs in many years. For example, an individual who has not been smoking tobacco for a few years can experience cravings to smoke when returning to an old house where they used to smoke (NIDA, 2020).
Tolerance
Tolerance refers to the “requirement for increasing doses or quantities of alcohol or other drugs in order to create the same effect as was obtained from the original dose” (Fisher & Harrison, 2017). Tolerance occurs when the brain adjusts to the high levels of dopamine or other transmitters triggered by a substance by producing less or reducing the number of receptors. As a result, levels of transmitters can become abnormally low and the individual has to increase the amount of substance taken to achieve the same effect. Typically, tolerance is the first sign of physical dependency,
Many drinkers mistakenly believe that building up a tolerance or increased ability to consume alcohol means they are somehow at less risk of developing alcohol dependency. However, studies indicated that a high metabolic and physiological tolerance actually yields a greater risk for alcohol dependency (Shilling et al., 2020).
Withdrawal
Substance withdrawal refers to the “physical and psychological effects that occur when a drug-dependent individual discontinues alcohol or other drug use” (Fisher & Harrison, 2017). Most withdrawal symptoms are the opposite of the drug effect (Shilling et al., 2020). For example, cocaine withdrawal is characterised by psychological depression, irritability, and extreme fatigue (Abadinsky, 2014). Another common example of withdrawal symptoms is a ‘hangover’ the day after a night of heavy drinking – although this is mild in nature it is a symptom of the body’s withdrawal from alcohol. Of course, withdrawal symptoms typically get worse with increasing levels of dependence. In fact, withdrawal from chronic alcohol use is actually one of the most life-threatening types of withdrawal, with nearly 15% of alcohol-dependent individuals experiencing withdrawal seizures if not medically detoxified (Shilling et al., 2020).
You will learn more about the withdrawal symptoms of each drugs in the later part of this section. Now that you have a basic understanding of the neurophysiology of drug use and addiction, let’s briefly explore some other factors that need to be considered in order to understand drug effects on individuals.
Read
Reading B: Effects of Drugs on Brain Structure and Function: The Exposure Model
Reading B provides an overview of the neurophysiology of addiction. It looks at the effects of drugs on brain structure and how drugs affect brain function.
Reflect
As you complete this reading, reflect on the following questions:
- Why do some individuals turn to AOD for gratification and pleasure?
- Are there any alternatives to AOD for gratification and pleasure?
Factors that Influence Substance Effects

Despite understanding how drugs affect our brains through neurophysiological studies, substances can have different effects on individuals depending on the three primary factors below:

For example, two individuals taking the same dosage of the same type of drugs might experience different drug effects due to other factors. Below are some of the example factors categorised based on the primary factor (Adapted from Department of Health, 2004; YouthAOD Toolbox, n.d.):
Drugs
- Dosage (quantity/amount of drugs used): Drugs can be taken in a range of doses – from low (i.e., no detectable effect), to moderate (i.e., producing the drug’s desired effect), to large and unpleasant (i.e., leading to a possible overdose).
- Method of administration: Drugs can be taken via a range of methods, such as inhalation, injection (intravenously), snorting/snuffing, and ingestion. Drugs that are inhaled, injected intravenously, or smoked can reach the brain almost instantly, hence producing an immediate response on the individual. The intensity of injected drugs may be stronger than that of inhaled drugs as more of the drug reaches the brain.
When a drug is snorted (taken through the nose), it is absorbed through the mucus membranes that are lining the nasal passage, thus producing a weaker intensity as the drug takes longer to reach the brain.
Oral ingestion (or swallowing) is another method to administer drugs. Drugs taken this way enter the bloodstream more slowly than other methods as the body has to metabolise them before reaching the brain. Different methods of drug administration will have different intensity and duration of a drug’s effect (see diagram below):
For example, methamphetamine can be administered in different ways: snorted, smoked, injected, or ingested orally. If the individual smoke or inject the drug, they will experience an intense rush or “flash” almost immediately. This “flash” lasts for a few minutes. When snorted, methamphetamine produces feelings of euphoria within three to five minutes; when ingested orally, it produces effects within 15 to 20 minutes. The “flash” that resulted from snorting is not as intense as the effect resulted from injection or smoking (NIH, 2020). - Poly drug use: It is the use of two or more types of drugs, administered either at the same time or sequentially. This includes the use of illicit drugs as well as over-the-counter medication and prescribed drugs. Past research has shown that compulsive individuals may use more than one drug to either enhance or moderate the effects of the primary substance (Alcohol and Drug Foundation [ADF], 2020, Abadinksy, 2014).
For example, individuals who use heroin often administer cocaine and alcohol together with heroin; individuals who use cocaine may use alcohol or sedatives to alleviate the unpleasant side effects of cocaine (Abadinksy, 2014). The use of multiple substances can influence their drug effect on the individual’s body and are often dangerous and unforeseeable. - Onset: How soon are the drugs felt?
- Intensity: How strong are the effects?
- Duration: How long do the effects of the drug last?
- Type of drug: Different types of drug elicit different responses and has different amounts of time which the drug effect lasts.
- Purity of drug
- Time taken to consume
User
- Age: Individuals who are younger or older than average (i.e., children and older adults, respectively) tend to have higher sensitivity to drugs than average adults.
- The individual’s past drug experience
- Tolerance of the drug: (including intoxication, aftereffects, and withdrawal) – Individuals who are exposed to certain drugs continuously tend to increase the drug dosage to get the desired initial drug effects.
- Gender
- Body weight (including amount of muscle): Individuals whose body weight is lighter than average may only be able to take lesser amounts of a drug compared to someone who is heavier. This is because the proportion of the drug in their blood system will be more.
- Mood or attitude: Current mood and psychological health of the individual
- Expectations and beliefs of drug effect: Individuals who believe they are drinking an alcohol drink when in fact, is a non-alcoholic drink, may still react and experience the effects of alcohol.
- Rates of absorption and metabolism: Individuals who have higher metabolism rate might metabolise the drug faster and thus may not experience any or less intense drug effects than others; if individuals have lower metabolism rate the drugs may slowly accumulate to toxic levels.
- General health: Any existing medical conditions (e.g., disease and allergy) can interfere with the body’s ability to handle any unexpected and unintended drug effects.
Environment
- Social setting: The presence of other people and who they are to the individual can affect the effect of drug taken. For example, an individual who consumes alcohol with friends at a music festival may experience strong effect of alcohol compared to when they drink alone at home.
- Physical setting: The noise level, size of the space, brightness of the space can influence drug effect. For example, a setting whereby a noisy house party is held compared to a dimmed and quiet bedroom)
After learning about the factors that can influence drug effects on individuals who use AOD, it is also crucial you to understand the various types of drugs and their impact on the individual’s body. For the remainder of this section, we will be exploring the most commonly used drugs in Australia and their effects.
Reflect
Try to recall a time whereby you (or someone you know) experienced an unexpected effect from a drug. Briefly reflect on the experience and list down any factors that you think could have contributed to experiencing the undesired drug effect.
In that situation, was there any other individual who consumed the same dosage of the same substance? If so, did two individuals experience the same effect?

There are many different types of drugs that are being circulated in our community and more are emerging. A good way to keep track of them for medical, treatment, and legal purposes is to have a drug classification system by organising the drugs into different categories. However, there is no one standardised drug classification system being used. In other words, the same drug may be classified differently under two different systems (Juergens, 2020). Below are a few most commonly used drug classification system:
- Effects of the drugs on the Central Nervous System: This is one of the most common classification system whereby drugs are categorised based on their influence on the individuals’ mind and body.
- Chemical similarities of the drugs: Drugs that are chemically similar often have similar impacts and risks on individuals. For example, an individual who has dependency on a certain drug is more likely to become dependent on another drug that is chemically similar.
- Legal status of the drugs: Most countries’ legal system would have a legal classification system for drugs to determine where a specific drug is legal, illegal, or decriminalised. This classification system is often based on the risk and danger of a drug as well as its perceived medical value.
- Uses of the drugs: For medicinal or recreational purposes
- Source of the drugs: Is the drug synthetic or obtained from plant?
- Risk status of the drugs: Is it considered dangerous or safe?

According to the Department of Health (2019b), in Australia, drugs are typically classified according to their effects on an individual’s CNS (mind and body). The brain is the major part of the CNS and where drugs have their main effect on. The following are the six categories of this drug classification system:
- Depressants: These substances slow down the activity and function of the CNS, which creates a calming or sedating effect (thus, also known as relaxants or “downers”). This does not mean that the individual will feel depressed after administering depressants into their body.
- Stimulants: These substances speed up the activity and function of the CNS by increasing the processing rate of the system. They are also known as “uppers”, and typically provide the individual a “rush”.
- Opioids/Narcotics: Similar to depressants, opioids are substances that slows down the activity and function of the CNS, thus slowing down the messages between the brain and rest of the body. These substances act through opioid receptors by affecting the opioid receptors in the brain. Opioids are often used to treat pain as they are able to alter the perception of pain and bring about a long-lasting euphoric state followed by drowsiness and relaxation. Therefore, opioids are often used due to its ability to manipulate the brain’s reward pathway.
- Hallucinogens: These substances are sometimes known as “dissociatives” or “psychedelics”. They can alter the individual’s perception of reality (e.g., thoughts, moods, sense of time) and often result in auditory and visual hallucinations. This process is often known as “tripping”, and is caused by distorting the messages carried in the CNS.
- Cannabinoids: These substances refer to any substances (medicinal, recreational, or synthetic) that joins the cannabinoid receptors of the body and the brain. They typically have a similar effect to cannabis (also known as marijuana), which leads to a “high”. These substances have the properties of both hallucinogens and depressants – when administered, the individual may experience happiness, relaxation, quietness, and more.
- Inhalants: Inhalants include a wide range of chemicals that are administered primarily by inhaling them, or huffing. Despite the variety of substances, most of them produce a pleasurable effect on the individual, also known as a “high”. Most of these substances are commonly available materials in our everyday life and not meant to be administered into our body.
Depressants
Depressants are often used as medications for some mental health conditions and sleep deprivation as it creates a relaxing feeling and induces sleepiness. After administering these substances, individuals typically experience a euphoric feeling, which led to it being one of the most commonly used substances as individuals long for the euphoric state. However, depressants are highly addictive and also have highly dangerous effects and likely to cause an overdose. Below are some of the most commonly used depressants:
Alcohol
Alcohol has been around for a long time and humans have been using it for thousands of years due to its intoxicating and relaxing effects. As alcohol is easily accessible and used widely throughout the world, it is one of the most commonly used drug. In 2017-2018, nearly 4 in 5 Australians aged 18 years and above consumed alcohol in the past 12 month (Australian Institute of Health and Welfare [AIHW], 2020). Given the prevalence of alcohol consumption in Australia, as helping professional, you must be ready that you will engage with people who uses alcohol in a frequent manner (Teeson et al., 2012).
Alcohol is typically consumed orally as a drink in the form of wine, beer, or hard liquor. Alcohol, or known as ethanol (ethyl alcohol) by its chemical name, is actually the substance in these drinks that influences your behaviour and mood (e.g., drunk). Ethanol is made by yeast fermenting the sugars in grains, fruits, and vegetables, e.g., vodka is made from the sugar in potatoes. Some alcoholic drinks are stronger (i.e., higher concentration of alcohol) than other drinks; see below for the alcohol concentration of different alcoholic drinks:
- beer contains 0.9% to 6% alcohol
- wine contains 12% to 14%
- fortified wines such as sherry and port contain 18% to 20%
- spirits such as scotch, rum, vodka and bourbon contain 40% to 50%
(Department of Health, 2019a)
Because of the different alcohol concentrations in different drinks and come in different sizes, it may be difficult for someone to measure how much alcohol they have consumed. Hence, a standard drink guide is made available for individuals to keep track of how much alcohol they are actually drinking.
Find Out More
Are you aware that you can compare the number of standard drinks you consumed against the Australian guidelines to reduce health risks from drinking alcohol?
Australian guidelines to reduce health risks from drinking alcohol is developed by the National Health and Medical Research Council (NHMRC) is used to reduce health risks from drinking alcohol by providing everyone in Australia with evidence-based advice on health effects of consuming alcohol, including advice on how much alcohol should be consumed.
Alcohol is a controlled and legal drug (depressant). Even though in small amounts alcohol can induce feelings of relaxation and happiness, people who use alcohol consistently and have their life negatively impacted by alcohol are considered to experience alcohol (mis)use. Even if the alcohol concentration are low, drinking alcohol is never free of risk. A survey by the Australian Institute of Health and Welfare (2020) reported that over 2 in 5 adults aged 18 years and above drank more than 4 standard drinks in a single occasion, exceeding the single occasion risk guidelines (i.e., no more than 4 standard drinks on any one day). They also reported that in 2017-2018, an average of 2.72 standard drinks per day were consumed by per alcohol consumer aged 15 and above. This shows the high prevalence of alcohol consumption in the Australian community.
So what exactly happens after all these alcohol are consumed?
As alcohol is consumed, it is absorbed directly into the bloodstream through the stomach and small intestine walls, and travels to all parts of the body including the brain, where the main effect of alcohol takes place. It will then slow down your brain and influence almost all parts of your body and the way you think, feel, and behave. Additionally, when you consume alcohol, your blood alcohol concentration (i.e., the level of alcohol in your blood) increases. For example, when a healthy person consumes one standard drink, their blood alcohol concentration increases by about 0.02, meaning there is 0.02g of alcohol in 100ml of their blood. However, remember that drugs has varied effects on different persons, thus the increase of blood alcohol concentration may be different for everyone (Department of Health, 2019a).
While most alcohol in the individual’s body is removed by the liver, small amounts of them are excreted from the body through perspiration, breath, and urine. Our liver can only metabolise alcohol at a rate of one standard drink (i.e., 10g of alcohol) per hour, which again, varies drastically according to the individual’s sex, weight, and overall health. In other words, it can take up to hours for the individual to remove any effects of alcohol. Though widely believed, alcohol cannot be removed from our blood by drinking coffee or vomiting and the only way to lower the blood alcohol concentration is time.
As mentioned, alcohol has been consumed by humans for thousands of years and it has established its importance as a social and cultural tool in Australia (AIHW, 2020). Indeed, when consumed in moderation, such as following the drinking guidelines, individuals may experience very minimal harmful impacts from alcohol. However, when alcohol is consumed frequently in an excessive manner (i.e., alcohol use), it can bring about harmful effects on the individual and their community. Below are the few categories of alcohol use:
- Hangover: Consuming alcohol excessively (both short- and long-term consumption) typically causes hangover. Signs include headache, dehydration, feeling ill, nausea, shakiness and, tiredness. This depends on how the individual’s body process alcohol and varies between different people. For example, some people may experience hangover after just one standard drink, while others may drink six standard drinks and not experience a hangover at all.
- Binge drinking: Drinking heavily over a short period of time. Typically, men who consume five or more alcohol drinks, women who consume four or more over two hours, are considered binge drinkers. Individuals who binge drink usually intend to get severely intoxicated quickly. In the long run, individuals who do not seek help or try to cease binge drinking may develop long-term alcohol dependency. There are also many short-term problems that are associated with binge drinking:
Physical effects: Immediate and severe intoxication, lack of coordination, sleepiness, dehydration, headaches, shakiness, dizziness, nausea, diarrhoea
Behavioural effects: Risk taking behaviour, vomiting, slurred speech, aggressiveness
Cognitive effects: reduced concentration, forgetfulness, distorted perception, increased confidence
Affective effects: mood changes (e.g., from happy to sad and back to happy again), remorse, guilt. - Alcohol poisoning: People who binge drink also are at risk of alcohol poisoning. This occurs when the blood alcohol concentration is extremely high that it affects the individual’s breathing and/or consciousness. This is extremely dangerous as it is associated with the risk of breathing and/or heart rate slowing down and approaches coma or death. If the individual becomes unconscious, they are also at risk of choking on their own vomit, or sometimes, though rarely, their tongue.
- Long-term alcohol dependence: moderate to heavy regular drinking over a long period of time. Individuals typically display signs of craving for alcohol and no signs of ability to cease alcohol consumption despite causing severe personal or social harm. This is also known as alcohol addiction or alcoholism (however, keeping in line with a person-centred approach, it is preferred to use the term ‘dependence on alcohol’).
Individuals may also display withdrawal symptoms when stopping alcohol consumption. Their thoughts are often consumed by alcohol and unable to perform personal and professional responsibilities. Individuals may also experience physical dependence whereby their body is used to functioning with alcohol in their body and now without alcohol, may experience difficulty to function normally. In the long run, this can have irreversible harm on their CNS and liver. Other effects from long-term alcohol dependence include:
Physical effects: Tremor/shakiness of hands, nausea, sweating, headaches, cramps, convulsions, twitching of muscles, rapid heart rate, increased blood pressure, pancreatitis, gastrointestinal problems, fatty liver, cirrhosis, Wernick’s encephalopathy, Korsakoff syndrome
Behavioural effects: Difficulty sleeping without a drink, insomnia, irritability, inability to maintain employment, aggressiveness, loss of interest in food, reluctance to leave house, decreased libido
Cognitive effects: Delusions, hallucinations, memory loss, blackouts, distorted perceptions, confusion/ inability to focus
Affective effects: Anxiety, depression, paranoia, panic attacks, apathy
Individuals with long-term alcohol dependence often suffer from a range of health issues. One of these is thiamine (Vitamin B1) deficiency. Thiamine is necessary for all tissue development and maintenance, including brain tissue. Problems associated with tissue damage are Wernicke’s encephalopathy and Korsakoff’s syndrome. While these are two separate syndromes, more often than not one will lead to the other; hence, they are often referred to as Wernicke Korsakoff’s Syndrome (Abadinsky, 2014). Wernicke’s encephalopathy causes paralysis of the nerves that move the eyes (oculomotor disturbances), uncoordinated muscle control and difficulty walking. Individuals may also exhibit slurred speech, difficulty swallowing, and confusion.
In long-term alcoholism, steatosis (fatty liver) can also develop, causing the liver to enlarge. Alcoholic hepatitis is also quite common amongst heavy drinkers, causing acute abdominal pain, swollen liver and vomiting which can lead to jaundice, bleeding and liver failure (Abadinsky, 2014).
Most individuals who consumes alcohol regularly can develop a tolerance to its effects. According to Abadinsky (2014), alcohol converts to acetaldehyde, a toxin which could build up and permanently damage the liver. Acetaldehyde also crosses the blood-brain barrier, combining with neurotransmitters to produce tetahydrisoquinolines (TIQs), which attach to CNS receptors and produce a morphine type effect. The brain cell membranes then become abnormally thick. This reduces functioning and causes withdrawal symptoms when alcohol consumption ceases. Hence, it is the brain cells that actually become addicted to alcohol.
Someone who is dependent on alcohol will start experiencing withdrawal symptoms within 4 to 24 hours of their last drink. Symptoms fall into three categories:
- Autonomic hyperactivity: Sweating, Tachycardia (racing heart), hypertension (high blood pressure), tremors, fever, dehydration, and electrolyte imbalances
- Gastrointestinal features: Loss of appetite, nausea, vomiting, dyspepsia, diarrhoea
- Cognitive and perceptual changes: Poor concentration, anxiety, psychomotor agitation, disturbed sleep, vivid dreams, seizures, hallucinations, delirium
(Adapted from Badii, 2018)
Individuals with a high level dependence on alcohol can experience a severe alcohol withdrawal syndrome that includes symptoms such as seizures, hallucinations, and delirium tremens (DTs). It can also lead to death.
Lastly, because alcohol is so commonly available today, it is often used alongside other drugs. Because alcohol is a depressant, it has a severe risk when taken with other drugs of the same class, e.g., benzodiazepines and some painkillers. Consuming excessive alcohol alone can lead to death, but consuming it with other drugs exacerbates the risks and can be lethal in a short time after administration (Juergens, 2021).
Prescriptive Sedatives
Sedatives are prescribed medication that can slow down the individual’s brain activity and are usually prescribed to patients to make them feel more relaxed. Similar to alcohol, these substances have the ability to suppress brain activity. All sedatives lead to changes in mood, and impairment of psychomotor and cognitive functions, depending on the dosage. Low doses cause mild sedation and display symptoms such as antianxiety or tranquilising effects. Moderate doses of sedatives often lead to impairment in motor function, slurred speech, and gross changes in mental status and behaviour.
Lastly, large doses administered can lead to unresponsive stupor, respiratory depression, and possibly death.
The two most commonly used prescriptive sedatives are:
Barbiturates
The barbiturates, originally introduced into clinical medicine in the early 1900s, were thought initially to be safe and effective agents for treating anxiety and insomnia, but were later found to have a high potential for dependence and particularly lethal in terms of overdose, especially when combined with alcohol.
(Washton & Zweben. 2008, p. 47)
Barbiturates are often referred to as ‘sedative-hypnotics’ as they depress the CNS and sensory cortex, causing drowsiness, mild sedation, hypnosis, and/or deep coma. They came to prominence in the 1960s and 1970s when they were often used medically for the treatment of anxiety, insomnia, and some types of seizure disorders (Abadinsky, 2014).
However, they are both psychologically and physiologically addictive and many individuals started to use them recreationally for their ability to decrease anxiety, reduce inhibitions, and treat unwanted side effects from other illicit drugs. While barbiturates can be injected, they are usually taken in pill or capsule form, and are often referred to as “downers’ or “barbs”. Sometimes they are known by the colours of their brand name versions: blues or blue heavens (Amytal), yellow jackets (Nembutal), red birds or red devils (Seconal), and rainbows or reds and blues (Tuinal; Abadinsky, 2014).
Generally, small amounts of barbiturates produce calmness and muscle relaxation. In some individuals, however, barbiturates may have a stimulating effect when taken in small doses – the environment and the individual’s expectations can play a significant role in the perceived effects. Larger doses can cause slurred speech, staggering gait, poor judgement, and slow uncertain reflexes. Large doses can cause unconsciousness and death.
Long-term use of barbiturates can cause depression, aggression, mood swings, chronic fatigue, lapses in memory, impaired judgement, and could prompt the emergence of symptoms of pre-existing emotional disorders (Abadinsky, 2014).
With continuous use of barbiturates, tolerance builds quickly but not uniformly, with individuals developing tolerance to certain effects of the drug faster than other effects. This makes increasing one’s dosage a dangerous practice. For example, while an individual may have built a tolerance to the sedating or euphoric effects of the drug, they may not have built a tolerance to the respiratory depressant effects, leading to unintentional overdose (Doweiko, 2015). Accidental deaths are not uncommon because the lethal dose of a barbiturate remains similar regardless of tolerance (Doweiko, 2015). Additionally, in some cases, because of the effects of barbiturates, individuals can forget that they have taken the drug and take even more, resulting in overdose.
Withdrawal from barbiturates is similar to alcohol withdrawal, with symptoms including confusion, muscle weakness, hypotension, loss of appetite, muscle twitches, anxiety, agitation, and delirium. These withdrawal symptoms typically develop 2 to 8 days after the sudden stop of administering barbiturates. Seizures and death can occur, which is why withdrawal should occur only under a doctor’s supervision. Generally speaking, longer-acting barbiturates will have longer periods of withdrawal (Doweiko, 2015).
Due to concerns regarding accidental deaths associated with barbiturates, benzodiazepines are now more commonly prescribed to treat problems like anxiety and insomnia. The potential for addiction and overdose still exists with benzodiazepines, but the risks are greatly reduced.
Benzodiazepines
Benzodiazepines are depressants drugs (also known as minor tranquilisers) primarily prescribed to treat anxiety and insomnia. Prescriptions used to treat anxiety and stress are called anxiolytics (i.e., tranquilisers); the ones prescribed legally to treat insomnia/sleeping problems are sedatives or hypnotics. Benzodiazepines are also prescribed to treat epilepsy and withdrawal symptoms from other depressants such as alcohol. However, benzodiazepines are generally prescribed for short-term use to prevent individuals from getting addicted to it.
There are three types of benzodiazepines: short-acting, intermediate-acting, and long-acting. Benzodiazepines that are short-acting have stronger withdrawal effect and can be more addictive than the long-acting benzodiazepines. This depressant drug is produced by a range of different pharmaceutical companies and thus have different chemical and brand names. Below are the chemical names and brand names of a few most commonly used types of benzodiazepines:
| Chemical Name | Brand Names |
|---|---|
| Diazepam | Valium, Ducene |
| Alprazolam | Xanax, Kalma, Alprax |
| Oxazepam | Alepam, Murelax, Serepax |
| Nitrazepam | Alodorm, Mogadon |
| Chlordiazepoxide | Librium |
| Temazepam | Euhypnos, Normison, Temaze |
| Flunitrazepam | Rohypnol |
Each benzodiazepines has their own unique function. For example, Valium is prescribed for individuals to experience a feeling of calm and well-being to relieve stress; but after using for an extensive periods it can produce severe and intense secondary anxiety. Despite the majority of benzodiazepines being legally prescribed, there is still a black market for the drugs to be traded illegally. One of these drugs is Rohypnol (chemical name: flunitrazepam). It dissolves readily when mixed with carbonated drinks and the individual will experience blackout (anterograde amnesia) for many hours. It is very commonly used as a tool for sexual assault, thus it is also widely known as the “date rape” drug.
The majority of benzodiazepines are in the form of pills or tablets for oral consumption; however, sometimes people also inject benzodiazepines. For example, Valium also comes in the form as a clear and odourless liquid. When it enters the individual’s body, it binds with GABA receptors, which is a special neuron, and reduce the brain’s overactive function. As a result, the individual will experience a feeling of relief from the mental stress they were having. When taken, individuals experience a euphoric “high” or “buzz”, and followed by a prolonged sedation (Juergens, 2021). Below are some other short-term effects of using benzodiazepines, which may vary among the individuals due to different factors we discussed:
- Relaxation, sleepiness, and lack of energy
- Dizziness
- Euphoria
- Confusion
- Visual distortions
- Moodiness
- Short-term memory loss
- When taken intravenously, it may cause vein damage and scarring, infection (e.g., hepatitis B, hepatitis C, HIV, and AIDS), deep vein thrombosis and clots
When individuals take benzodiazepines regularly (i.e., use), they may develop benzodiazepines dependency, which impose longer-term effects on individuals, including serious medical implications, such as:
- Anxiety, irritability, paranoia, aggression, and depression
- Muscle weakness, rashes, nausea, and weight gain
- Sexual problems
- Menstrual irregularities
- Memory loss, cognitive impairment, dementia, and falls
- Confusion, lethargy, and sleep problems
(AIHW, 2020)
When individuals reduces the use or dosage of benzodiazepines significantly, they tend to experience withdrawal symptoms, which vary between individuals. However, some withdrawal symptoms can sometimes turn deadly when the intake of benzodiazepines are stopped abruptly, due to the high risk of seizures, coma, and even death. Hence, it is a safer choice to consult a health professional and decrease the dosage gradually. Below are some withdrawal symptoms that the individual may experience:
- Headaches
- Aching or twitching muscles
- Dizziness and tremors
- Nausea, vomiting, and stomach pains
- Poor concentration
- Anxiety and irritability
- Delusions, hallucinations, and paranoia
- Seizures
Individuals who use the drug over a very long period of time may develop tolerance towards the drug, i.e., taking higher dosage to achieve the initial euphoric state. This may eventually lead to intentional or accidental overdose. In 2018, benzodiazepine was the most common drug present (51%) out of the 1,740 drug-induced deaths in Australia (AIHW, 2020). Some of the overdose symptoms includes over-sedation or sleep, slow and shallow breathing, unconsciousness or coma.Some individuals might mix benzodiazepines with other depressants such as alcohol to boost the euphoric feeling from benzodiazepines. Of course, by mixing the drugs, it will increase the risk of lethal overdose due to individuals unable to predict the effects of poly drug use. Also, some individuals use benzodiazepines to help with the come down effects of stimulant drugs and this may lead to a cycle of dependence on both types of drugs.
Stimulants
Stimulants work by increasing the speed for transmitting messages from the brain to the body, which leads to feelings of alertness and well-being, confidence and with more energy. This is achieved by increasing the amounts of the neurotransmitters (dopamine and norepinephrine) in the brain. These chemicals helps to improve the brain’s concentration and decrease the tiredness of the individual’s body.
Cocaine
Cocaine is extracted from the leaves of the coca bush (Erythroxylum coca) which is native to South America. Coca leaves are pulverised and added with chemicals to obtain a crude crystalline substance, coca paste. This paste is then dissolved with hydrochloric acid which presents in the form of a white crystalline powder, known as cocaine hydrochloride. This is the purest form of cocaine, but it is usually diluted, or “cut” before being sold on the street to increase its sale profit. Neutral substances such as lactose or talcum powder are usually used to mix it, but it might also be mixed with other drugs. Typically, street cocaine has around 20% purity, but it may be as high as 50% as well, which may potentially lead to cocaine overdose for unsuspecting individuals (Abadinsky, 2014). Cocaine is also commonly known as coke, blow, powder, C, nose candy, Charlie, and stardust on the streets.
Cocaine is most commonly snorted (i.e., inhaling it up the nose) by individuals, which takes around 10 to 15 minutes for any noticeable drug effects to take place; peak effects usually take place within 30 to 60 minutes after intake. Some individuals may dissolve cocaine powder in water to form cocaine hydrochloride solution and consume it intravenously via a syringe. It can also be smoked with other drugs such as tobacco or marijuana. Smoking and injecting cocaine lasts for a shorter period compared to snorting it, about 5 to 10 minutes, but it produces a more intense experience.
In 2020, 4.2% of people aged 14 and above in Australia reported that they have used cocaine in the last 12 months; and 11.2% of people reported use of cocaine at least once in their life (AIHW, 2020). Even though cocaine affects every individual in different ways, those who take a lower dose of cocaine typically experience the following short-term effects:
- Sense of euphoria and wellbeing
- Increased blood pressure, heart rate, and body temperature
- Increased alertness and energy
- Sexual arousal
- Loss of appetite
If higher dosages are taken, individuals who use cocaine can experience megalomania (obsessive desire for power) and feelings of omnipotence (having unlimited or great power). Individuals who use high-dosage cocaine may also experience cocaine psychosis – including paranoia, hallucinations, unusual thoughts, and out of character behaviours. These symptoms usually lasts for a few days or weeks after the cease of cocaine use. After that, individuals go through a “coming down” period, and may feel the following:
- Irritability and paranoia
- Mood swings
- Feeling uncomfortable
- Exhaustion
The feelings individuals experience during the coming down period has a stark difference compared to the “euphoric high” they experience when using cocaine. Thus, they tend to dose frequently in order to maintain that effect and eventually, may develop a dependence on cocaine. It is extremely difficult for someone who is addicted to cocaine to overcome it because they need to use cocaine in order to feel normal. It is also because the drug increases the brain’s dopamine level to an abnormal level, which ultimately reprograms the brain reward system.
When individuals develop cocaine addiction, they may experience the following long-term effects:
- Sleep disorders
- Sexual problems such as impotence
- Nose bleeds, sinusitis, and damage to the nasal wall from snorting
- Cardiovascular problems and stroke
- Paranoia, depression, and anxiety
- Cocaine-induced psychosis
Overdose occurs when the individual takes a large amount or have a strong batch of cocaine. They typically experience symptoms such as: nausea and vomiting, extreme anxiety, panic, hallucinations, kidney failure, stroke, seizures
Individuals who decide to cease cocaine use usually go through a challenging phase, especially for those who used cocaine for a long time. This is because the individual’s body has gotten used to functioning with cocaine in its system. However, some individuals who had a short binge may also experience withdrawal symptoms. Some of the withdrawal symptoms (usually start around 6 to 12 hours after last use), categorised into three phases, are listed below (adapted from Alcohol and Drug Foundation, 2019):
- Crash: feelings of depression or anxiety, cocaine cravings, extreme tiredness (typically in the first few days)
- Withdrawal: cocaine cravings, lack of energy, anxiety, agitation, disturbed sleep, and an inability to feel pleasure (typically lasts for several weeks)
- Extinction: withdrawal symptoms can occur over several months (typically gradually subsiding)
Cocaine and alcohol are frequently used together to extend the “high” from cocaine and to reduce the withdrawal effects from “crash”. Individuals may also take cocaine together with heroin in the same syringe, which is known as “speedballing”, in an attempt to reduce the undesirable side effects from both drugs. Once again, the poly use of cocaine and other drugs often result in unpredictable and unpleasant reactions, particularly lethal overdose (Washton & Zweben, 2008).
Amphetamine
Amphetamine is a synthetic stimulant that increase activity of the central nervous system and make people feel alert and energetic, and sometimes staying awake for 2 to 3 days or longer. Amphetamine is shortened from alphamethlphenethylamine; it is also known as speed, up, uppers, rack, whiz, etc., on the streets. Certain types of amphetamines are legally prescribed for conditions such as Attention Deficit Hyperactivity Disorder (ADHD) and narcolepsy (uncontrollable urge to sleep). Outside of legally prescribed drugs by medical professionals, amphetamines are produced and sold illegally, which sometimes are taken as performance enhancement drugs.
Amphetamines come in various different forms: powder (range of colour including white, brown, and may have pink and grey traces), tablets, crystals, and capsules. They have a very strong smell and bitter taste. When traded illegally, amphetamine comes in “foils”, whereby they are packaged in aluminium foil, or sometimes in plastic bags or small balloons. Amphetamine might be mixed with other substances such as other drugs, sugar, and caffeine when it is produced illegally (ADF, 2019).
These drugs are typically swallowed, injected, smoked, or snorted. Individuals experience the effects of amphetamines either immediately (if smoked or injected), or within 30 minutes (if snorted or swallowed). The common experiences are listed below:
- Happiness and confidence
- Becoming more talkative and feeling energetic
- Large pupils and dry mouth
- Increased heart rate and breathing rate
- Teeth grinding
- Reduced appetite
- Increased sex drive
- Increased risk of violent behaviour
- If snorting: nasal passage is damaged and nose bleed
- If injecting: increased risk of tetanus, infection, vein damage and blood clots
When amphetamines are used for an extended period of time, individuals may experience the following:
- Reduced appetite and extreme weight loss
- Restless sleep
- Dental problems
- Regular colds and flu
- Depression, anxiety, and paranoia
- Increased risk of stroke
- Tolerance and dependence on amphetamines
- Financial, work, and social problems
If a strong batch of amphetamine is taken in high dosage, the individual may overdose and experience any of the following symptoms:
- Increased and racing heartbeat
- Fits
- Passing out or having difficulty to breathe
- Chills or fever
- No urine output
- Stroke, heart attack, and death
After using amphetamine, in 2 to 4 days, individuals go through a “coming down” period and may experience the following:
- Restless sleep and exhaustion
- Headaches
- Paranoia, hallucinations, and confusion
- Twitching and muscle aches
- Fluctuating temperatures
- Irritability, mood swings, anxiety and depression
Individuals who decide to stop using amphetamines may experience the following withdrawal symptoms:
- Cravings for amphetamines
- Increased appetite
- Confusion and irritability
- Aches and pains
- Exhaustion, restless sleep, vivid dreams, and nightmares
- Anxiety, depression, and paranoia
Similar to cocaine, sometimes amphetamines are taken together with other drugs (including legally prescribed drugs). As with other poly drug use, this can be extremely dangerous as the individual may experience unpredictable and undesired symptoms. For example, when an individual takes amphetamine with alcohol, the individual experiences an increase in heart rate and blood pressure (ADF, 2019).
Methamphetamines
Methamphetamine is also known as methylamphetamine, with common street names such as ice, meth, crystal, chalk, and crank. Similar to amphetamine, it is also a stimulant, but more concentrated, and thus, has a stronger drug effect on individuals. It can be made easily from relatively inexpensive and ingredients that are available over-the-counter. Methamphetamines used to be a legally prescribed medication for weight loss and decongestant. However, many used it for the stimulant effects and thus, it is now classified as an illegal drug; but one prescription drug is still used to treat obesity and severe ADHD.
Methamphetamine comes in different forms and most commonly found as meth and crystal meth. Meth is a white crystalline powder (sometimes yellow, pink, or brown) and it is odourless and bitter. It is administered by smoking, snorting or dissolving it in water and injecting it; though sometimes individuals compressed the powder into a pill and swallow it. Crystal meth, or ice, on the other hand, is clear or with blue coarse crystals and usually smoked.
This drug is highly addictive and may cause addiction just after one use in some individuals. Similar to cocaine, the methamphetamines produce a high amount of dopamine in the brain, which induces a pleasurable feeling in the individual and experiences a euphoric state. However, it has a longer stimulant effect compared to cocaine as it stays unchanged in the body for a longer period of time. In other words, 50% of cocaine is removed from the body within an hour while 50% of methamphetamine is removed from the body within 12 hours. Not only that, methamphetamine’s “high” lasts around 6 to 8 hours but cocaine’s only lasts for minutes.
Sometimes, the drug is “cut” with other drugs such as alcohol, morphine, and Xanax. For example, individuals take methamphetamine with morphine (a type of opioids) as this poly drug use creates a greater “high” than either drug can create on their own. However, this use also increases the risk of an overdose.
Individuals usually take the drug over a period of several days, also known as “binge and crash”, whereby the individual consume a great dose of methamphetamine (“binge”) until they run out of supply or collapse from extreme physical exhaustion (“crash”). Some of the short-term effects that can be observed and experience are (adapted from AIHW, 2020):
- Increased in energy
- Sense of euphoria and well-being
- Increased attention, alertness, and talkativeness
- Increased heart rate, breathing, and body temperature
- Decreased appetite
- Nervousness, anxiety, and paranoia
- Aggression and violence
Individuals who use the drug on a regular basis may eventually develop the following long-term effects:
- Mood and anxiety disorders
- Cardiovascular problems
- Haemorrhagic stroke
- Psychotic symptoms such as paranoia and hallucinations – some individuals might develop “ice psychosis” when high doses are used frequently and it usually disappear a few days after they stop using ice
- Chest pains
Other than the health effects that the individual may experience, there are also social costs such as with the criminal and justice system. According to the AIHW (2020), 51% of the police detainees in 2019 were tested positive to methamphetamine. Additionally, in the previous section you’ve learned about other social costs inflicted by drugs use. In 2013-2014, the estimated social costs of methamphetamine use in Australia was over $5 billion (AIHW, 2020). This shows that the use of methamphetamine not only has its impact on the individual themselves, but also those around them in the community.
Similar to most drugs, individuals who use methamphetamine regularly can rapidly get addicted to it and develop a dependence on it. They typically feel the need to use methamphetamine before performing daily activities such as studying, working, and socialising. This makes it more difficult for individuals to stop the use of methamphetamine. As such, there is a chance that the individual can overdose when a large amount or strong (higher purity) batch of methamphetamine is taken, and may experience any of the following symptoms:
- Increased heartbeat and chest pain
- Difficulty breathing
- Extreme agitation, confusion, and clumsiness
- Sudden and severe headaches
- Unconsciousness
Individuals who have decided to stop the use of methamphetamine may experience the following withdrawal symptoms, which usually appears on the first or second day without use:
- Increased in appetite
- Aches and pains
- Exhaustion
- Anxiety, depression, and paranoia
- Cravings for methamphetamine
Ecstasy (MDMA)
Methylenedioxymethamphetamine (MDMA) is a stimulant drug that has similar chemical properties to methamphetamine but also has hallucinogenic properties. It is more commonly known as ecstasy, molly, pills, and pingers. MDMA was first produced in the early 1900s and was initially used to help facilitate psychotherapy sessions by helping clients gain insights into their emotions. However, it became popular in the 1970s as a recreational drug (or “party drug”).
It comes in the common form of pills or tablets; it is usually swallowed but can be crushed up and snorted, and though rarely, sometimes inserted as a suppository (inserted through the rectum). The tablets often come in different colours and sizes and logos, symbols, or have pictures imprinted on them. It is important to note that even though two pills have the same appearance, they may have different effects as they can have different ingredients and come from different sources. For example, some pills sold have very small amount of MSMA in it while some pills have other drugs or “fillers” instead.
When consumed, MDMA produces a feeling of happiness and friendliness. The drug increases the release of the neurotransmitters serotonin (the “happy” brain chemical) and dopamine – it produces a drug-induced “high” (Abadinsky, 2014). The drug also enhances the individual’s five senses. When taken, the effects produced by MDMA kicks in around 20 minutes to an hour; the effects of MDMA lasts for around 3 to 5 hours, depending on a variety of factors. The following are some short-term effects of MDMA (adapted from AIHW, 2020):
- Sense of euphoria and well-being
- Feelings of intimacy with others (including peacefulness, acceptance, and empathy)
- Confidence and lack of inhibitions
- Increased blood pressure and pulse rate
- Nausea and sweating
As mentioned, ecstasy is often mixed with other drugs by the sellers and may have very little to no MDMA in the pills. As such, individuals who wish to achieve the same MDMA effect, may have to take a higher dosage of the drug and thus, leading to a high possibility of overdose. Individuals who take a higher dosage may experience floating sensations, perceptual changes (such as visual and auditory hallucinations), out-of-character irrational behaviour, high body temperature and convulsions (uncontrolled muscle contractions).
When MDMA are used regularly, individuals may experience the following:
- Colds or flu
- Depression and anxiety
- The need to use more MDMA to achieve same effect
- Memory and concentration problems
Withdrawal symptoms usually disappear around a week after the individual stops using MDMA and mostly disappears after a month. Some withdrawal symptoms include aches and pains, exhaustion, restless sleep, agitation, trouble concentrating, and cravings for MDMA (ADF, 2019). As MDMA is usually used in episodic or specific social situations (often at parties, clubs, or raves), individuals rarely develop compulsive use or addiction to it. However, sometimes an ecstasy addiction may not be recognised immediately because the withdrawal symptoms are not as obvious as other substances (Juergens, 2021).
Nicotine
Nicotine is a stimulant drug derived from the leaves of the tobacco plant and it is the addictive active ingredient found in tobacco products. The leaves are dried, cured, and aged before other ingredients are added to produce the different tobacco-based products. It is a colourless liquid that turns yellowish brown when it is smoked by the individual and acquires the smell of tobacco when exposed to the air (Washton & Zweben, 2008).
Tobacco-based products such as cigarettes, cigars, and pipes are typically smoked, but it can also be chewed and snorted. There is also a recent increase in the use of electronic cigarettes (also known as “e-ciggies”), a device that delivers nicotine and other chemicals through aerosol vapour that the individual inhales. In 2016, AIHW (2020) reported that 1 in 3 current smokers aged 14 and above have used e-cigarettes. In other words, e-cigarettes appear to be the emerging new drug that is commonly used among the youths.
However, while it is legal to use tobacco in Australia, it is illegal to sell e-cigarettes that contain nicotine in Australia other than for personal therapeutic purposes (AIHW, 2020). Because tobacco use in Australia is legal and it is readily available, there is a high use of tobacco-based products in the country: 11.0% of persons aged 14 and above reported that they smoke daily (AIHW, 2020).
When inhaled, nicotine will be absorbed in the mucous membranes, lungs, and bloodstream and then into the brain. Similar to other stimulants, some CNS receptors have a liking for nicotine. They trigger the release of stimulating neurotransmitters and also indirectly increase the release of dopamine. As a result, individuals experience a stimulant effect within 10 seconds of inhaling nicotine. It is important to note that the effects are different among people, especially whether the individual normally smokes tobacco products. People who do not frequently smoke tobacco products experience the following:
- Dizziness
- Headache and nausea
- Abdominal cramps
- Possibly vomiting or weakness
However, people who smoke tobacco products regularly tend to build up a tolerance towards nicotine, and instead, experience the following immediate short-term effects (adapted from ADF, 2020):
- Mild stimulation
- Increased heart rate
- Increased ability to concentrate
- Relaxation
- Coughing
- Bad breathe
- Reduced appetite, stomach cramps, and vomiting
- When taken in large amounts, individuals may experience confusion, feeling faint, seizures and respiratory arrest (cease of breathing) and death.
There are various long-term health effects due to the regular smoking of tobacco products, including chronic disease and issues, such as stroke, pneumonia, diabetics, and reduced immune function. Further, AIHW (2020) reported that tobacco was the leading cause of cancer in Australia in 2015. This shows that using tobacco has a wide range of health effects on individuals. Other than the health costs inflicted upon the individual, the community also suffers from the impact of tobacco use. For example, AIHW (2020) reported an estimated social cost of $136.7 billion in 2015-2016.
Withdrawal from nicotine is often challenging for individuals who use it long-term because they usually have developed a dependence on it to function daily. Thus, many individuals who attempted to quit tobacco relapsed (Washton & Zweben, 2008). The withdrawal symptoms usually start within 2 to 3 hours after the last use of tobacco and may last from a few days to a few weeks. These symptoms include cravings for tobacco products, restless sleep, eating more, weight gain, headaches, and aches and pains.
It was not until recent times that the discussion of tobacco-based dependence or addiction have been discussed. This is because compared to other stimulants like cocaine or ecstasy, there are no observable changes in behaviour, personality, and affect. However, most people who are addicted to using nicotine still continue to use despite being aware of its harms; hence, it is also considered as an addiction (Juergens, 2021). Luckily, there are now more acknowledgement in the treatment of nicotine dependency. Thus, as a helping professional, you need to be aware that nicotine addiction should be given the same awareness and treated the same as other stimulant drug dependencies.
Opioids/Narcotics
Opioids are drugs (natural, semi-synthetic, or synthetic) that are derived from the plant opium poppy (Papaver somniferum). Below is an extract from Washton and Zweben (2008) about the history of opioid use:
Opioid use has been known to have occurred throughout recorded human history, dating back to references to “poppy juice” in the third century B.C. Smoking opium was widespread during the late part of the 19th century and early part of the 20th century in the United States among Chinese immigrants, but it was the invention of the hypodermic needle, combined with the use of morphine to treat wounded Civil War soldiers.
(Washton & Zweben, 2008, p. 58)
In other words, opioids are one of the most effective pain relievers, and are often prescribed to patients who are experiencing mild to severe pain. When the dosage taken is high enough, individuals can also relieve themselves from emotional and psychological pain. This is achieved when opioids bind to the opioid receptors, which then depresses the CNS and reduces the speed of messages sent between the brain and the rest of the body. As a result, the individual will experience a decreased heart rate and breathing rate. Further, the receptors also stimulate the release of dopamine, which results in individuals experiencing feelings of pleasure and pain relief (Juergens, 2021).
Opium
Opium is a sticky gum that has a dark-brown colour and a strong odour. Opium is derived from the opium poppy which is one of the earliest medicinal plant. Its medicinal use can be dated back to 3, 400 BCE, which was cultivated by the Sumerian people.
It is relatively easy to process opium for use. The poppy seed pod is first lanced so that the milky white latex that the pod holds is able to exude from it. The substance will then be dried and left for it to semi-solidify overnight. It will then be scraped off on the following day and typically refined further by boiling and drying it (usually now in powder form). When in powder form, it can be smoked or ingested orally (mixed with liquid or added to food). Nowadays, opium is usually harvested to be processed into other stronger drugs.
After taking opium, individuals typically experience euphoria, relaxation, decreased heart rate, impaired reflexes, loss of appetite, and more. In a longer run, the regular use of opium will lead to individuals developing tolerance, constipation, and dependence on opium. Females may have irregular periods and experience difficulty having children. Because opium has a strong relaxing effect, individuals might not even know that they overdose. Overdose symptoms include very slow breathing, loss of consciousness, and tiny pupils. If left untreated, it can lead to brain damage and death.
Withdrawal symptoms typically occurs between 6 to 24 hours aft the last opium use, and lasts around 7 to 10 days. The withdrawal symptoms can be described as flu-like, such as restlessness and irritability, insomnia, diarrhoea, muscle cramps, fast heartbeat, and more (ADF, 2019).
Morphine
Morphine is used to relieve severe pain and can provide a euphoric feeling which is often described as a dreamlike state. It usually can be taken orally as a tablet or syrup, injected, or smoked. The tolerance to morphine can develop quickly and thus it has a high risk for individuals to develop a morphine dependence Individuals tend to use morphine due to the feelings of pleasure and the ease of accessing it. Also, any use of morphine without a prescription (i.e., non-medicinal purposes) is also considered as morphine use (Juergens, 2021).
Heroin
Heroin is synthesised from morphine and it is highly addictive. Initially, heroin was used for medicinal purposes and was sold in cough suppressants and other medication. However, by mid 1920s, heroin was illegal in most countries due to the rate of usage. Heroin is also known as H, junk, the dragon, and dope.
Heroin has several different forms but the most common three forms are fine white powder (purest form), brown or black powder (more common than white powder heroin; colour obtained from the additives), and black tar heroin (black sticky gel). Heroin is usually melted from crystal or powder form and injected, but can also be smoked (“chasing the dragon”), and snorted.
The effects of heroin are almost instantaneous – typically within seconds – when injected or smoked; when snorted, the effect takes around 10 to 15 minutes to come into effect. Individuals typically experience the following short-term effects which lasts around 3 to 5 hours:
- Analgesia (the inability to feel pain)
- Euphoria (intense pleasure and pain relief)
- Dry mouth
- Feelings of detachment
- Reduced appetite and vomiting
- Decreased sex drive
- Heavy feeling in hands and feet
- Severe itch
- Cough suppressant
When heroin is administered for a long time, individuals may experience the following long-term health effects:
- Severe constipation
- Tooth decay (due to lack of saliva from dry mouth)
- Irregular menstrual periods in females
- Impotence in males
- Memory impairment
- Physical dependence and associated withdrawal that may manifest as flu-like symptoms
As heroin is highly addictive, it is very challenging for an individual to quit heroin and not relapse. In 2019, 43% of people who used heroin reported that they have tried to stop or cut down heroin use but failed to do so (AIHW, 2020). Again, this shows that heroin is highly addictive and not easy to quit. Individuals who just started using heroin may enjoy the pleasurable feelings from heroin because it does not produce any significant come down effect from the initial use like cocaine. As a result, they may perceive that it is harmless to use heroin and may eventually develop dependency on heroin. In a long run, the individual may develop tolerance and increase their doses which ultimately leads to lethal heroin overdose. AIHW (2020) reported that the risk of overdose for heroin is high and has been increasing in the recent years, and heroin accounts for 25% of drug-induced deaths in Australia in 2018.
Withdrawal symptoms from heroin usually starts 6 to 24 hours after the last heroin dose and lasts for around 7 to 10 days. Typically the first 3 days will be the toughest. The symptoms include: cravings for heroin, anxiety, depression, crying, diarrhoea, restless sleep and yawning, vomiting, and no appetite.
Codeine
Codeine is a prescribed medication and is usually prescribed by medical professionals as a pain reliever to treat mild to moderate pain, diarrhoea, and dry irritating cough. Codeine is also the main ingredient in prescribed cough suppressants. Sometimes, the use of cough suppressants leads to the individual developing a tolerance towards codeine and eventually an addiction to it. It is also combined with other medications to provide relief from certain conditions. For example, codeine can be combined with paracetamol or aspirin to provide relief from severe pain; when combined with antihistamines and decongestants, it helps with cold and flu.
Because codeine is readily available over the counter, it has become the most commonly used opioids in Australia, including non-prescribed use as coping mechanism to cope with chronic pain and depression and anxiety. This prompted the regulatory body to cease its over-the-counter availability (Cairns et al., 2019).
This drug usually comes in different forms such as tablets and capsules and taken orally. However, it can also come in the form of suppositories, liquids, and soluble powders and tablets, which will be dissolved in water and injected into the individual’s body. After administering codeine, the individuals typically experience the following symptoms:
- Dizziness and tiredness
- Confusion and difficulty concentrating
- Euphoria
- Restlessness
- Blurred vision and dry mouth
Individuals who take codeine regularly may experience the following symptoms:
- Constipation
- Reduced sex drive
- Tension and muscle twitches
- Financial, work, and social problems
As mentioned earlier, individuals tend to administer a higher dosage to achieve the same initial effect from codeine. As a result, they may experience overdose from codeine, which includes the following symptoms:
- Inability to pass urine
- Agitation
- Severe constipation and obstructed bowel
- Mental numbness
- Hallucinations and sometimes seizures
- Coma and death
Withdrawal symptoms of codeine includes seeking for codeine containing medicines, dilated pupils, lack of appetite, flu like symptoms, goosebumps. In order to achieve a more intense “high”, individuals tend to take codeine with other drugs such as alcohol, which can cause mental clouding, slow breathing, and reduced coordination. Because both alcohol and codeine has depressant properties, this poly drug use can be extremely dangerous as it greatly depresses the activity in the CNS.
Methadone
Methadone is also a prescription drug like codeine. However, it is typically taken as an alternative for heroin or other opioids during treatment for dependence on these drugs. This process is known as pharmacotherapy – replacing a dependence drug with a prescribed drug to help reduce harms related to drug use. Methadone is also used to relieve pain from heart attacks, trauma, and surgery.
Similar to other opioids, methadone interacts with the opioid receptors in the brain and elicits a range of responses within the individual’s body, including relaxation, pain relief, contentment, and pleasure (ADF, 2019). Because it interacts with the same receptors as other opioids such as morphine and heroin, it helps to minimise and stabilise withdrawal symptoms. Further, methadone is a synthetic drug and is designed to block the feelings of pleasure that is brought upon by other opioids.
In Australia, methadone is only legally available via treatment programs to assist with opioid dependence. Typically, an individual who wishes to reduce their dependence on heroin will be assessed by a General Practitioner who has registration as a methadone prescriber. For the duration of the treatment program, the individual/patient will then visit a pharmacy to receive a daily dose of methadone. It is typically in syrup form; however it may be injected or swallowed as tablets when it is for pain relief treatment (ADF, 2019).
There are many advantages of using methadone to control the withdrawal symptoms from other opioid use. For example, it is highly unusual for patients to overdose when they use methadone on its own. Also, because methadone is typically taken orally, it reduces health problems, especially when those which are injection-related, such as HIV, skin infections, and vein problems (ADF, 2019).
Typically, a single dose of methadone lasts around 24 hours, compared to a dose of heroin, which lasts around a couple of hours. Even though it is much safer to take methadone than other opioids, there are still some common side effects such as sweating, difficulty passing urine, loss of appetite, nausea, constipation, lethargy, mental clouding, and confusion. Additionally, patients on the treatment program may experience some undesired symptoms at the beginning before determining the right dosage for them. If the dosage is too low, patients may experience runny nose, yawning, back and joint aches, cravings for the dependence drug(s), and more. On the other hand, if the dosage is too high, patients may experience depressed breathing, stupor (state of near-unconsciousness) or coma due to accumulation of the drug, intense red rash with itching or hives, collapse, and more.
When used for an extended period of time, methadone does not cause any physical harm to the individual. Even when taken in its purest form, it does not cause damage to the individual’s major organs (ADF, 2019).
Find Out More
Naloxone is a drug that can temporarily reverse the effects of opioid overdose or severe reaction. Naloxone can be administered by injecting or delivering through a nasal spray. When overdosed, the user will most likely be unable to talk, or even unconscious, therefore, unable to administer naloxone themselves.
According to previous reports, opioid use is a major cause of hospitalisation and death in Australia. Thus, the Australian Government invested in the “Take Home Naloxone Pilot”, whereby people who are likely to experience or witness an opioid overdose are able to obtain naloxone for free, and no prescription is required.
Hallucinogens
Hallucinogens have been around since the ancient times and has been used in different cultures for religious and healing purposes. However, with emerge of the psychedelic culture in 1960s, more people have been using it for recreational purposes, such as “tripping” (being under the influence of a hallucinogen). However, they are usually not taken regularly but only during specific occasions, which are usually weeks or months apart. Hallucinogens can be obtained naturally such as from the trees, vines, and fungi, or synthetically made in laboratories (ADF, 2019; Juergens, 2021).
When taken, hallucinogens, or “psychedelic drugs”, are able to alter the individual’s perception of reality, such that the individual see, feel, and hear things that are not real. Sometimes, the individuals are not able to correctly interpret what is going on around them when under the influence of drugs. These can be categorised into three main symptoms:
- Depersonalisation: out of body experiences where the mind seems to have detached itself from the body
- Synaesthesia: seeing sound and hearing visual input
- Hallucinations: perceiving sounds, odours, tactile sensations or visual images that came from internal stimuli (rather than external stimuli)
Hallucinogens can also magnify the individual’s affectivity and may lead to drastic changes of mood. For example, the individual might feel depressed or anxious but turn euphoric, or vice versa. Hallucinogens target specific areas of the brain and alter how the brain understands sensory input. These drugs distort the messages between the CNS and the body, thus the brain is unable to correctly modulate any sensory input.
LSD (Lysergic Acid Diethylamide)
LSD is a synthetic drug made from substances found in ergot (a fungus that infects grain). It is also commonly known as acid, trips, tabs, or Lucy. When LSD is in its pure state, it appears like a white crystalline substance and is odourless. Typically, this drug is diluted with other material because in its pure state, an effective dose is very small and virtually invisible. Drops of LSD solution are dried onto gelatin sheets, blotting paper pieces or sugar cubes. The individual will then swallow it or put it under the tongue to dissolve it, whereby the drug will then be released from the sheet and absorbed in the bloodstream. LSD can also come in the form of liquid, capsules, or tablets and can be sniffed, injected, or smoked (ADF, 2019).
The effects of LSD appears within 30 to 40 minutes after consumption and lasts around 8 to 12 hours. Individuals may experience the following effects:
- State of euphoria and well-being
- Dilation of pupils
- Changes in perception, including auditory and visual hallucinations
- Confusion and trouble concentrating
- Increase in body temperature
- Facial flushes, sweating, and chills
Some individuals may experience “bad trips” whereby they have disturbing hallucinations. This can be dangerous as it can lead to dangerous and risky behaviours. For example, someone might experience a hallucination of a ghost chasing after them and run across the road to escape from it.
Though it is uncommon, there are some people who use LSD regularly, and in the long run, they may experience flashbacks. This is when an LSD experience reoccurs and typically they are visual distortions with perceptual or emotional changes. There is no set amount of time in which the individual may experience flashbacks, it can happen anywhere between weeks to years after the last dose of LSD was taken. Flashbacks can be brought on when the individual takes other drugs, experiences stress or tiredness and they last for a couple of minutes.
When the individual takes a higher dose of LSD, they may experience overdose and display symptoms such as panic, paranoia, psychosis, and increase in risk-taking behaviours. There are no known physical withdrawal symptoms of LSD, as LSD dependence does not happen among regular individuals. Tolerance to LSD effects develops very quickly. After the third or fourth consecutive days of taking LSD, no dosage of the drug can produce any desired effects. But, when the use of LSD is ceased for a few days, the normal tolerance returns.
Sometimes, LSD is taken with other drugs such as ice or ecstasy. This can lead to an increased chance of a bad trip and may lead to panic. Alcohol and LSD is another popular combination of poly drug use, and this may lead to an increase in feelings of nauseas and vomiting (ADF, 2019).
PCP (Phencyclidine)
PCP is a dissociative anaesthetic that induces a trance-like state and feelings of being “out of body” or detached from the environment. PCP has been used as an anaesthetic in veterinary medicine, but never approved for use in humans because of the adverse reactions that arose during clinical trials, including extreme agitation and dysphoria experienced by patients emerging from anaesthesia.
(Washton & Zweben, 2008, p. 66)
PCP is a mind-altering drug that may lead to hallucinations in individuals. As mentioned in the extract, because of its extremely neurotoxic side effects, it was never developed further for human use. PCP is also known as rocket fuel, love boat, ozone, angel dust, or superweed.
PCP in its pure state appears as a white crystalline powder which can be dissolved readily in alcohol or water. However, when sold illegally, it is typically mixed with a number of contaminants. This changes its colour, ranging from light to dark brown and its consistency from powdery to a gummy mass consistency. It also comes in liquid form. PCP can be taken through snorting, smoking, injecting, or swallowing the drug.
When taken, the effects of PCP lasts for 4 to 6 hours. Typically, PCP causes the following effects in individuals:
- Euphoria
- Relaxation
- Drowsiness
- Dissociation
- Trouble concentrating
- Hallucinations
- Blurred vision
- Dizziness
- Impaired motor skills
- Muscle rigidity
Because PCP is fat soluble and stored by fat cells, the body can hang on to it longer compared to other drugs. However, this means that in individuals with higher body fat, the effects of PCP can fluctuate over a few days to months. In other words, when the individual experiences an increase in body temperature, the drug that is leftover in the body may become reactive, causing flashbacks in the individual.
When individuals take high dosage of PCP, it can cause seizures, coma, and death (typically due to accidental injury or suicide during PCP intoxication). Those who regularly use PCP often develop dependence to it and experience symptoms such as memory loss, difficulties with speech and learning, depression, and weight loss (Santos-Longhurst, 2020).
Psilocybin (Magic Mushrooms)
Psilocybin is a hallucinogen that is extracted from certain types of mushrooms in South America, Mexico and the United States. Historically, it has been used by Indigenous communities in Mexico and Central America to connect to the spiritual world during religious ceremonies. It gained popularity in the 1960s and today, many use it for recreational purposes, such as at music festivals. Some other common names of magic mushrooms are shrooms and mushies.
There are various types of magic mushrooms and the most common ones in Australia are golden tops, blue meanies, and liberty caps (ADF, 2019). It appears like other ordinary mushrooms, but also similar to poisonous mushrooms which can lead to individuals who mistook it to become very sick and possibly even death. Magic mushrooms can be eaten raw, cooked, or brewed into tea. It can also be dried into white crystalline powder which then processed into tablets or capsules. In its powder form, it can be mixed with cannabis or tobacco, and then smoked.
Within 20 minutes to 2 hours after consuming magic mushroom, individuals tend to experience the following symptoms:
- State of euphoria and well-being
- Change in consciousness, mood, thought, and perception (“a trip”)
- Changes in perception
- Introspective or spiritual experiences
- Headaches, fast or irregular heartbeat
This happens because psilocybin is converted to psilocin in the individual’s body, and psilocin is the chemical with psychoactive properties. These effects typically lasts around 4 to 6 hours. For individuals who regularly use magic mushrooms, they may experience flashbacks whereby they relive the magic mushroom experience. Similar to LSD, these flashbacks can happen anytime between weeks to years after the last dose of magic mushroom is taken. Even though it is extremely uncommon for individuals to experience any life-threatening symptoms, they may still experience overdose when a strong batch of mushroom is consumed. Overdose symptoms include agitation, vomiting, muscle weakness, psychosis, seizures, and coma.
Some individuals take magic mushrooms with other drugs, such as with ice and ecstasy. This will increase the chances of a bad “trip” and can lead to panic. Some individuals on psychiatric medications might take their medications with magic mushrooms, which may lead to a relapse of the condition or worsen it (ADF, 2019).
Ketamine
Similar to PCP, ketamine is used by medical practitioners and veterinarians as an anaesthetic. Ketamine is also known as Special K, K, KitKat, Super K, and horse tranquiliser. This drug usually comes in the liquid form to be injected for legal medicinal purposes. However, when produced and distributed illegally, it usually appears as a white crystalline powder and can be made into tablets or pills. In this form, it can be swallowed or snorted or smoked with cannabis or tobacco (ADF, 2019; Juergens, 2021),
Due to ketamine’s psychedelic properties, some individuals use it to get “high”. Individuals experience its effects within 30 seconds if ketamine is injected, but up to 20 minutes if swallowed. The effects lasts around 45 to 90 minutes and these effects include:
- Feeling happy and relaxed
- Feeling detached from your body (“falling into a k-hole”)
- Hallucinations
- Slurred speech and blurred vision
- Anxiety, panic, and violence
- Vomiting
- Lowered sensitivity to pain
Individuals who has been administering ketamine regularly may experience headaches, flashbacks, poor sense of smell (due to snorting), poor memory, thinking and concentration, mood and personality changes, and depression. Additionally, individuals who take large doses of ketamine regularly may eventually develop ketamine bladder syndrome, which would require ongoing treatment. It is a painful condition which includes symptoms such as difficulty holding in urine, incontinence (accidental or involuntary loss of urine, flatus, or faeces). These symptoms can result in ulceration in the bladder.
As described above, “k-hole” is an experience whereby ketamine individuals have a near-death or out-of-body experience, often detached from the reality. Recall that drugs have different effect on different individuals, including the dose required to achieve the same effect on different individuals. Because of this, some individuals who attempt to experience “k-hole” can consume too much ketamine and lead to accidental overdose. Overdose symptoms include inability to move, rigid muscles, high body temperature and increased heartbeat, convulsions, coma, and death. Withdrawal symptoms typically persist around 4 to 6 days, and can include: cravings for ketamine, no appetite, tiredness, nightmares, anxiety, depression, and irregular and fast heartbeat.
When used with other drugs, the effect of ketamine is often dangerous and unpredictable. For example, taking ketamine and alcohol or opioids can result in vomiting, decreased breathing rate, coma, and death, as the individual may not be aware of the effects of depressant drugs. Another poly drug use is taking ketamine with amphetamines, ecstasy, and cocaine, which can lead to an enormous strain on the body and increased heart rate (ADF, 2020).
Cannabinoids
Cannabinoids refers to every chemical substance that is able to produce similar effects as the Cannabis Sativa plant. These chemical substances (mainly delta-9 tetrahydrocannabinol, or THC) work by interacting with the endocannabinoid system in the brain, which regulates various activities such as mood, memory, sleep, and appetite. They disrupt the cells in the system by slowing down the messages sent between the brain and the body, thus creating a feeling of relaxation and calm in the individual.
These drugs appear in different forms, such as cannabis, hashish, and hash oil. Recent years, the production and use of synthetic cannabis emerges, which attempts to reproduce the same effects as cannabis. This form of cannabinoids are more potent but also creates more adverse effects than cannabis.
Cannabis

The first use of cannabis can be dated as far back as 2727 B.C. after the discovery of tools used to burn cannabis - almost 5,000 years ago! Cannabis are often harvested from the two most common species – Cannabis sativa and Cannabis indica. This drug appears in various forms and the most common ones are:
- Herbal cannabis (Marijuana): It is the dried leaves and flowers of the cannabis plant and it is the most common but weakest form across all cannabis. It is usually grounded up and individuals smoke it in a cigarette (“joint”) or a pipe (“bong”).
- Cannabis resin (Hashish, or hash): It is the dried plant resin from the plant’s leaves and stems compressed into blocks. It is usually mixed with tobacco, sometimes with marijuana too, and smoked in cigarettes. Another common way of consuming hash is to mix it into food such as cookies and brownies.
- Cannabis oil (Hash oil): It is extracted from the hashish and appears as a thick oily liquid in a wide range of colour (e.g., golden brown or dark green). It is also the most potent form of cannabis and usually added sparingly to tip of a cigarette and smoked with tobacco.
In Australia, cannabis is the most widely used illicit drug. There also is a relatively high prevalence of individuals who use cannabis regularly, with 36% of recent cannabis users reporting at least weekly use in 2016 (AIHW, 2020). After consuming cannabis, it takes around 1 to 3 hours for the effect to take place. Individuals may experience short-term effects such as the following (AIHW, 2020):
- Mild euphoria, relaxation, and reduced inhibitions
- Perceptual alterations, including time distortion and intensification of ordinary experiences
- Feeling of hunger
- Panic reactions, confusion, and feelings of paranoia (usually by new and naïve individuals)
- Nausea, headache, and reddened eyes
- Increased heart rate for up to 3 hours after smoking
- Dizziness, impaired balance and coordination
When an individual takes cannabis for a prolonged period, they may develop tolerance to the effects of cannabis, dependence on cannabis, and reduced cognitive functioning. Smoking cannabis regularly may also increase the likelihood of individuals experiencing sore throat, asthma, bronchitis, and cancer (if smoked together with tobacco).
Even though there is a very low risk of overdosing on cannabis, individuals with high risk of mental illnesses such as bipolar disorder or schizophrenia are advised to not use cannabis. Specifically, individuals who are predisposed to psychosis may increase their risk of experiencing cannabis-induced psychosis.
Withdrawal symptoms include anxiety, irritability, loss of appetite and upset stomach, sweating, chills and tremors, and restless sleep and nightmares. These symptoms typically lasts for a week but the individual’s sleep can be affected for longer than that.
Medicinal Cannabis
Cannabis can be taken either recreationally, such as what you have learned above, or prescribed by medical practitioners for medicinal purposes, such as relieving symptoms of epilepsy. Currently, there is a legislation that has been passed by the federal government that permits the cultivation of cannabis for medical and/or scientific use in Australia. The Narcotic Drug Amendment Bill 2016 regulates and ensures that the cultivation, production, and manufacture of cannabis in Australia remains compliant with its international obligations (ADF, 2019).
Find Out More
Did you know that each jurisdiction has their own regulatory framework on regulating medicinal cannabis? Some states have established centres for research purposes to further understand cannabis and its effects on users.
Find out more about the situation in your state: Framework on regulating medicinal cannabis.
Butane Hash Oil
Butane hash oil is also known as BHO, dabs, or dabbing, Marijuana wax, and honeycomb. It is a highly concentrated substance that involved using butane oil to extract oils from the cannabis through a chemical process. It has a highly concentrated amount of THC (the main psychoactive chemical in cannabis), which is around 80%, compared to cannabis which has around 10-25%.
Butane hash oil can be consumed by using a specifically designed “bong” (or “oil rig”) to heat the drug and then smoke it. Some individuals prefer to dab the butane hash oil rather than smoking it, as it requires fewer number of times to take the drug to achieve a “high”. Due to its higher potency, there is a greater risk for individuals to develop a stronger tolerance towards butane hash oil, as well as experience more severe withdrawal symptoms. For example, when taking butane hash oil, individuals may experience pain relief, anxiety and panic, reduced attention rate, decreased reaction times, and detachment from reality.
Synthetic Cannabis
Synthetic cannabis is one of the more commonly used drugs, with 2.8% of Australians aged 14 and above reporting that they have used synthetic cannabis at some stage in their lives. Synthetic cannabis was originally produced to achieve a similar effect to cannabis. It is sold under different brand names with Spice as one of the earliest products sold. Other brand names include Kronic, Northern Lights, Mojo, Blue Lotus, and Godfather. It can also be marketed as aphrodisiac tea (increases sexual behaviour), herbal incense, and potpourri. Synthetic cannabis is typically smoked and sometimes drunk as a tea.
However, recent substances produced and sold as synthetic cannabis do not actually produce the psychoactive effects of THC. Further, it has been reported that synthetic cannabis produces additional negative effects on individuals compared to cannabis. These additional negative effects include racing thoughts, agitation, anxiety and paranoia, chest pain, aggressive and violent behaviour, acute kidney injury, seizures, stroke, and death.
Withdrawal symptoms include insomnia, paranoia, panic attacks, anxiety, mood swings, agitation and irritability, and rapid heartbeat. It is worth noting when regular breaks are taken when smoking the drug or using it at a lower dosage in one setting, the effects and risk of tolerance and dependence may be reduced (ADF, 2020).
Inhalants
Inhalants are volatile and often flammable substances that can produce vapours and fumes at room temperature. When taken, inhalants produce a “high” in individuals, similar to those of alcohol and marijuana, though more short-lived. Inhalants can be everyday household products such as glue, felt-tipped pens, or correction fluid (such as liquid paper). It can also be industrial products such as aerosol spray, chrome-based paint, petrol and medical products such as nitrous oxide. Inhalants are generally categorised into the following four categories (ADF, 2019):
- Volatile substances: These include industrial or household solvents or products containing solvents such as paint thinners or removers, degreasers, dry cleaning fluids, petrol, and glue.
- Aerosols: These include propellants and associated solvents such as spray paints, hair spray, deodorant spray, fabric protector sprays, aerosol computer cleaning products, and vegetable oil sprays.
- Gases: These include household or industrial items such as butane lighters, propane tanks, whipping cream aerosols (or dispensers), and refrigerant gases.
- Nitrites: These include things such as video head cleaner, room deodoriser, and leather cleaner.
The use of inhalants is relatively prevalent in Australia, especially among the adolescences. In 2014, a survey revealed that 15.9% of secondary school students (aged 12 to 17 years) had experience of using inhalants at least once. This poses a risk for these individuals as a study by Crossin et al. (2017) found that adolescent inhalant use is associated with the increased risk for subsequent and earlier onset of drug use. In other words, with the prevalence of inhalant use among Australian adolescences, it might bring about a higher prevalence of drug use in the future.
The most two common inhalant used are aerosol spray paint (chroming) and petrol sniffing. Inhalants are breathed in directly from the container or sprayed directly into the nose or mouth. Some individuals might spray them into a plastic bag, pour into a bottle or soak onto a cloth or sleeve before inhaling it. After inhaling, individuals experience the drug effects more rapidly compared to alcohol because the chemicals are absorbed into the blood through the lungs. These effects include:
- Intoxication
- Nausea and headaches
- Injuries
- Delirium
- Seizures
- Pneumonia from inhaling vomit
- Brain damage
- Coma and sudden death
- Asphyxiation (suffocation; if plastic bag was used)
Long term effects of regular inhalant use incudes: irritability and depression, memory loss, pale appearance, weight loss, reduced growth potential (Height), excessive thirst, liver and kidney damage, and dependence on inhalants. Even though most effects are reversible when the use is stopped, but some inhalants such as petrol can cause irreversible damage.
Further, there are some other factors that increase the risk when inhaling drugs such as sniffing in an enclosed space or indoors, doing physical activity after sniffing (can lead to death due to cardiac sensitisation), and mixing sniffing with medicines or illicit drugs. Though rare, chemicals in certain products such as aerosol sprays and model aeroplane cement can cause heart failure and thus sudden death.
Withdrawal symptoms start within 24 to 48 hours after the last inhalant use, and lasts around 2 to 5 days. These symptoms include hangover, tiredness, cramps, hallucinations and visual disorders (such as seeing spots), headache, and nausea (ADF, 2019).
As discussed earlier in this section, drugs can be classified in many different ways. The Drug Wheel is one of the ways to classify different drugs based on the effect they have on the individual’s body.
Do note that this drug classification system may differ slightly from the one that was discussed earlier in this section. However, the Drug Wheel (see diagram below; from ADF, 2019), still serves as a good quick guide about different types of drugs and their effects.

This section of the module gave you an introduction of the drug classification as well as different drugs that are most commonly used in Australia. This includes their prevalence rate, administration method, short- and long-term effects, overdose and withdrawal symptoms.
While you have learned a good deal about these different drugs, is important to remember that having substantial understanding of the different drugs will be extremely useful to you when working in this field.
The drugs mentioned in this module is not a comprehensive list of drugs available. It is also important to keep yourself updated with the new and emerging drugs in the Australian community. To do so, access information that are the most up-to-date and accurate via reliable and credible organisations such as AIHW and ADF.
Abadinsky, H. (2014). Drug use and abuse: A comprehensive introduction. Thomson Learning.
Alcohol and Drug Foundation. (2019, October 24). Drug Facts. https://adf.org.au/drug-facts/
Alcohol and Drug Foundation. (2020, January 3). Polydrug use. https://adf.org.au/reducing-risk/polydrug-use/
Australian Institute of Health and Welfare. (2020). Alcohol, tobacco and other drugs in Australia. https://www.aihw.gov.au/reports/alcohol/alcohol-tobacco-other-drugs-australia/contents/drug-types/alcohol
Badii, C. (2018, September 16). Alcohol withdrawal syndrome. Healthline. https://www.healthline.com/health/alcoholism/withdrawal
Cairns, R., Schaffer, A. L., Brown, J. A., Pearson, S.A., & Buckley, N. A. (2019). Codeine use and harms in Australia: Evaluating the effects of re-scheduling. Addiction, 115(3), 451-459. https://doi.org/10.1111/add.14798
Crossin, R., Cairney, S., Lawrence, A. J., & Duncan, J. R. (2017). Adolescent inhalant abuse leads to other drug use and impaired growth; implications for diagnosis. Alcohol, Tobacco, and Other Drugs, 41(1), 99-104. https://doi.org/10.1111/1753-6405.12595
Department of Health. (2004). 6.1 Factors influencing drug effects. https://www1.health.gov.au/internet/publications/publishing.nsf/Content/drugtreat-pubs-front6-fa-toc~drugtreat-pubs-front6-fa-secb~drugtreat-pubs-front6-fa-secb-6~drugtreat-pubs-front6-fa-secb-6-1
Department of Health. (2019a, February 26). About alcohol. https://www.health.gov.au/health-topics/alcohol/about-alcohol
Department of Health. (2019b, July 17). Types of drugs. https://www.health.gov.au/health-topics/drugs/about-drugs/types-of-drugs#:~:text=Drugs%20can%20be%20categorised%20by,of%20the%20central%20nervous%20system
Doweiko, H. E. (2015). Concepts of chemical dependency. Cengage Learning.
Juergens, J. (2020, December 2). Drug classifications. Addiction Center. https://www.addictioncenter.com/drugs/drug-classifications/
Juergens, J. (2021, March 25). Drugs. Addiction Center. https://www.addictioncenter.com/drugs/
National Institute on Drug Abuse. (2020, July). Drugs, brains, and behavior: The science of addiction. https://www.drugabuse.gov/publications/drugs-brains-behavior-science-addiction/preface
Santos-Longhurst, A. (2020, March 31). Everything you need to know about Angel Dust (PCP). https://www.healthline.com/health/pcp
Shilling, E. H., Veach, L. J., Rogers, J. L., & Moro, R. R. (2020). Substance addictions. In D. Capuzzi, & M. D. Stauffer (Eds.), Foundations of addictions counseling (pp. 23-50). Pearson Education.
Teeson, M., Hall, W., Proudfoot, H., & Degenhardt, L. (2012). Addictions. Psychology Press.
Washton, A. M., & Zweben, J. E. (2008). Treating alcohol and drug problems in psychotherapy practice: Doing what works. The Guilford Press.
Youth AOD Toolbox. (n.d.). Factors which influence drug effects. https://www.youthaodtoolbox.org.au/factors-which-influence-drug-effect
